Baseball, football and volunteer subjects have participated in the vision training program. All subjects have been college age men or women, between the ages of 18- and 26 years-old.
Football
The average *A score for 101 UC Football players the first time they performed it was 74.2 ± 10.3 hits per min (hpm) and the average Reaction Test time for their first time performing it was 0.34 ± 0.03 sec (n = 79, note not all 105 players had a chance to complete the Reaction Test).
Sixty-three players were exposed to multiple years of light board training. The players participated in training pre-season and weekly during the season for maintenance. The first *A run on for these players was 70.25 ± 9.61 hpm and significantly improved with training to 89.9 ± 10.5 hpm (p ≤0.01). Reaction Test results were 0.354 ± 0.034 sec and improved to 0.315 ± 0.031 sec after training; p ≤0.001. The average number of repetitions of the *A program per athlete among the entire group was 7.31 ± 9.12.
Table 1 consists of data for 63 UC Football players who had trained on the light board for over a minimum of three years. The table shows the average times it took for the players to hit the individual rings. The outer rings took longer times to hit as opposed to the rings in the center of the board, which is the center of the visual field.
Peripheral vision reaction time ratio can be calculated to determine a subject’s speed of reaction to what they see in their peripheral vision. The data collected during the *A session is used to calculate the average reaction time in the outer two rings of the vision board compared to the inner three rings. Each subject’s peripheral vision reaction time ratio from one training session to another is calculated as the ratio of the mean reaction times for the outer two rings divided by the mean of the reaction times for the inner two rings and provides a data point in addition to the average reaction time. A higher ratio means it takes longer to see and hit the buttons in the periphery compared to the center of the visual field.
Table 2 shows the average time it takes for 10 players to hit the different rings when they start the vision training pre-season7. Data reported for each subsequent year reported is for the players who completed the vision training program each year. At the beginning of the season the team’s intake values are repeated and tend to come to similar values for the first 3 years. After 4 years of vision training the sustained benefits of the training appear.
Table 3 consists of the first time on the system *A scores and Reaction Test scores broken down into groups based on years of play, positions, skilled or unskilled positions, or history of concussion16.
Volunteers
Table 4 summarizes the data collected from 20 non-football volunteers completing the three purpose built concussion programs (Concussion 1-3). These results of 10 men and 10 women volunteers represent normative data values for these more complex test programs. This reveals that with increased multi-tasking of the concussion tests there is no significant decrement in performance between Concussion 1 to Concussion 3. The slight increase in performance from Concussion 1 to 3 is also not significant, but could be an indication of a training effect.
Baseball
From the preseason (January) 2011 through to the end of the season (May) 2013 all hitters on the UC Division 1 Baseball Team underwent regular vision training. Out of season training was 20 min twice a week and in season was 20 min once per week. Traditional stereopsis (Stereo Fly) was performed and recorded. Players consistently presented with stereopsis ranging from 22 to 25 mm at the beginning of training. As a team they went back to this level consistently between seasons. Training increases this stereopsis effect. The 45 to 50 mm levels were consistently reached by the players during the season, data are in press.
Table 5 summarizes the average and standard deviation for the stereopsis measurements in mm for the UC Baseball Team as measured through the three years of vision training5.
| Variable | Ring 1 | Ring 2 | Ring 3 | Ring 4 | Ring 5 |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | |
| Average length of time to hit (seconds) | 0.52 ± 0.08 | 0.57 ± 0.11 | 0.62 ± 0.08 | 0.71 ± 0.09 | 0.81 ± 0.10 |
| Diameter of rings (inches) | 8.125 | 17.25 | 21.25 | 34.75 | 43.5 |
Table 1: Average length of time for hits per ring for the *A test for 63 UC Football players.
| Pre Season | Ring 1 | Ring 2 | Ring 3 | Ring 4 | Ring 5 | Functional Peripheral Vision Ratio |
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| 2010 | 0.56 ± 0.08 | 0.56 ± 0.06 | 0.69 ± 0.11 | 0.77 ± 0.12 | 0.98 ± 0.18 | 1.52 |
| 2011 | 0.62 ± 0.21 | 0.64 ± 0.19 | 0.72 ± 0.20 | 0.85 ± 0.26 | 1.02 ± 0.25 | 1.48 |
| 2012 | 0.55 ± 0.12 | 0.56 ± 0.12 | 0.64 ± 0.15 | 0.77 ± 0.20 | 0.91 ± 0.33 | 1.51 |
| 2013 | 0.52 ± 0.08 | 0.53 v 0.09 | 0.57 ± 0.07 | 0.67 ± 0.10 | 0.80 ± 0.19 | 1.4 |
Table 2: Average length of time (in sec) for hits per ring for the *A test per season of play (n = 10 each year).
| Results Based on Years of Play | |||
| Played college football > 2 years at time of testing | Played college football < 2 years at time of testing | P value | |
| A* (hits per minute) | 97.3 ± 12.18 | 92.0 ± 10.07 | ≤0.05 |
| (n=29) | (n=68) | ||
| Reaction Test (sec) | 0.33 ± 0.031 | 0.34 ± 0.038 | 0.26 |
| (n=29) | (n=65) | ||
| Results for Offensive versus Defensive Players | |||
| Defensive Player | Offensive Player | P value | |
| A* (hits per minute) | 94.5 ± 13.28 | 93.4 ± 8.97 | 0.31 |
| (n=42) | (n=55) | ||
| Reaction Test (sec) | 0.33 ± 0.033 | 0.34 ± 0.038 | ≤0.05 |
| (n=42) | (n=52) | ||
| Results Based on Skilled versus Non-skilled Positions | |||
| Skilled Position | Non-skilled Position | P value | |
| A* (hits per minute) | 93.8 ± 8.51 | 93.6 ± 12.75 | 0.45 |
| (n=45) | (n=52) | ||
| Reaction Test (sec) | 0.33 ± 0.040 | 0.34 ± 0.035 | 0.41 |
| (n=44) | (n=50) | ||
| Results Based on History versus No History of Concussion | |||
| History of Concussion | No History of Concussion | P value | |
| A* (hits per minute) | 96.3 ± 12.34 | 92.1 ± 9.19 | NS |
| (n=28) | (n=69) | ||
| Reaction Test (sec) | 0.33 ± 0.034 | 0.33 ± 0.036 | 0.39 |
| (n=27) | (n=67) | ||
Table 3: Best *A and best Reaction Test times sorted by years of play, position, skilled or unskilled position and history of concussion.
| Number of Hits per Minute | |
| Mean ± SD | |
| Concussion 1 Program | 88.4 ± 12.0 |
| Concussion 2 Program | 88.3 ± 11.6 |
| Concussion 3 Program | 90.4 ± 10.3 |
Table 4: *A results for 20 volunteers who completed the three purpose built programs: Concussion 1, Concussion 2, and Concussion 3.
| Season | Pre-Season | Start of Season |
| 2010 | ||
| Average (mm) | 22.7 | 36.5 |
| SD (mm) | 10.6 | 15.7 |
| t-Test | ≤0.0001 | |
| 2012 | ||
| Average (mm) | 23.6 | 36.7 |
| SD (mm) | 12.8 | 12.9 |
| t-Test | ≤0.01 | |
| 2013 | ||
| Average (mm) | 24.7 | 44.2 |
| SD (mm) | 12.9 | 8.6 |
| t-Test | ≤0.01 | |
Table 5: Stereopsis measured for UC Baseball players through the three years of vision training. Statistical significance is reported as p <0.05.

Figure 1: Subject demonstrating placement in front of the system and ready for the start of a program. (A) In front of the system. (B) Placement of hand to start the first test. (C) Hand sweeps left to the light that is lit.

Figure 2: Subject demonstrating Brock’s string method. (A) Focus on distant bead. (B) Focus on closest bead. (C) View from subject’s perspective.

Figure 3: Tachistoscope — photos from UC football games where subject is asked to re-call the numbers in the box plus elements of the photo like player number.

Figure 4: (A): pinhole glasses. (B) strobe glasses. Subject catching ball with strobe (C) or pinholes (D) glasses on.
Figure 5: Saccade chart.

Figure 6: Placement of charts for near far training (A). Subject demonstrating this method (B and C).
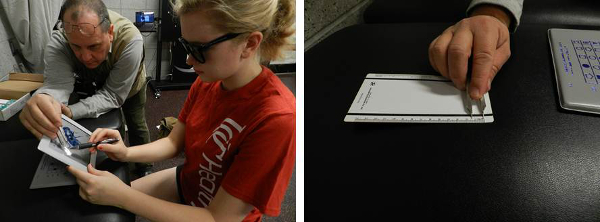
Figure 7: (A) subject pinching wing of Stereo Fly. (B) calipers used to determine the distance.
