The use of the autopsy samples and in vivo MR images for this protocol was in accordance with local regulations and approved by the local institutional review board of the University Medical Center Utrecht (UMCU).
1. MR-guided Histopathological Validation of Cortical Microinfarcts
- Ex vivo MRI
- When handling brain tissue, always wear gloves and suitable protective clothing.
- Based on the research question, select appropriate, preferably 10-mm thick, formalin-fixed brain slabs. The brain slabs for this paper were derived from the neuropathology department of the UMCU, and VU University Medical Centre (VUMC), based on known Alzheimer pathology.
- Formalin-fix whole brains for at least 3-4 weeks by immersion in 10% formalin, prior to cutting. Cut the brains into coronal slabs, containing both hemispheres.
- For post-mortem scanning, select for example three brain slabs per brain, taken from the frontal, temporo-parietal, and occipital regions of the brain. The current protocol is optimized for the use of three coronal brain slabs, containing both hemispheres, in one scan session.
- Take photographs of the brain slabs at both sides (dorsal and caudal), and take careful notes (or make sketches) of the orientation of the slabs in the container and in the scanner, for later co-localization of histology with MRI.
- Fill a purpose-built container (Figure 1) – in this case one that fits within the MR head coil – with 10% fresh formalin at RT. If MRI signal from the fluid is undesired, use a perfluoropolyether (PFPE) lubricant with a suitable density instead of formalin (such as Fomblin or Galden PFPE). Ensure to use a flow cabinet when handling formalin.
- When placing the brain slabs in the container, make sure to avoid air bubbles. Remove the majority of air bubbles by gently shaking the tissue, either by hand, or using a shaker or ultrasound bath.
- Make sure the slabs cannot move within the container and limit the amount of needed fluid, by using a smaller container to keep the slabs in place (Figure 1).
- Cover the container with plastic or parafilm, to prevent evaporation and to protect the MR (head) coil from potential contamination (Figure 2).
- Use a whole-body 7T MRI scanner with an appropriate coil. In this protocol a dual transmit and 32-channel receive head coil is used.
- Place the container in the head coil, wrapped in a towel or surgical underpad, to prevent potential spilling of fluid. Make sure the container cannot move, and that the slabs remain in horizontal position (Figure 2).
- Run a survey scan that can be used for the planning of the high resolution scans, correct B0 inhomogeneity by using an appropriate shimming tool, and calibrate the RF power to obtain the correct flip angles (the few slabs require less power compared to in vivo scanning of a whole head) according to manufacturer’s protocol.
- Plan the high resolution acquisitions on the survey scan, to ensure the brain slabs are fully included in the field-of-view. Scan the brain slabs O/N with the high resolution acquisitions shown in Table 1, which are optimized for ex vivo imaging. The acquisition protocol presented here includes a 3D FLAIR, T2, and T1 weighted image with an isotropic resolution of 0.4 mm, and a T2* weighted image with an isotropic resolution of 0.18 mm.
- Identify automatic software processes that may interrupt scanning, such as automated up-dates that run O/N, or warnings for peripheral nerve stimulation, and make sure the scanner procedures will not be interrupted by these.
- Monitor the scanner O/N for possible confirmation pop-ups that may interrupt scanning, by using for example a VPN connection.
- Return the following morning (after a total scan time of approximately 12 hr in the current protocol). Store the brain slabs in formalin, clean up.
- Save the images to an external hard disk.
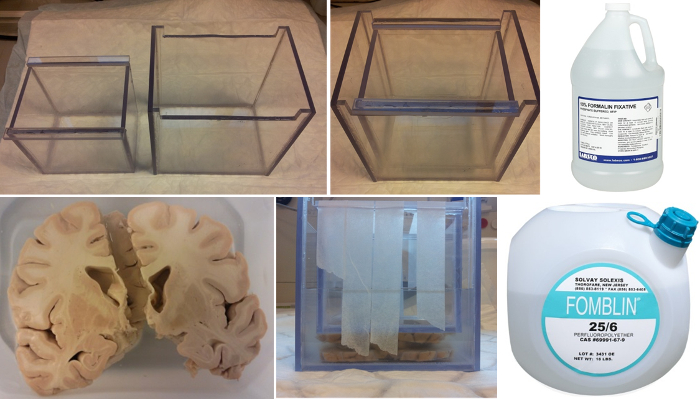
Figure 1. Preparation of formalin-fixed brain slabs for post-mortem scanning at 7T MRI. A purpose-built Perspex container is filled with either 10% formalin or a perfluoropolyether (PFPE) lubricant if MRI signal from the fluid is undesired. Three 10-mm thick formalin-fixed coronal brain slabs are placed in the container. A smaller container is used to keep the slabs in place. Tape the second container to the first one, to prevent movement.
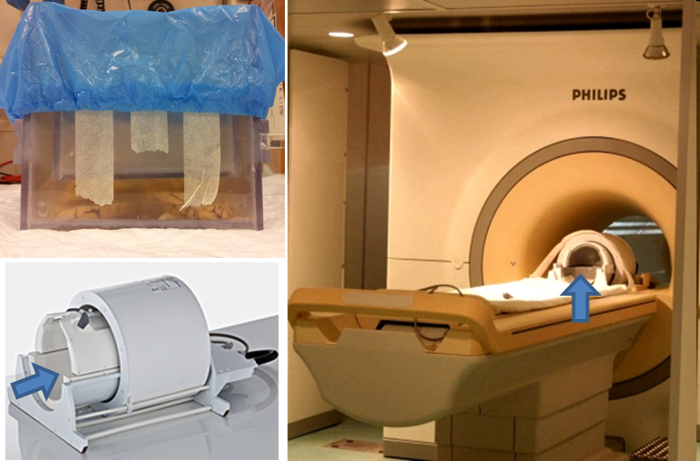
Figure 2. Placement of purpose-built container in 7T head coil. Cover the container with plastic or parafilm to prevent evaporation of the formalin. Place the container, enclosed in a towel or surgical underpad, in the head coil of a 7T MR scanner. Make sure the container cannot move, and that the slabs remain in horizontal position.
- Histopathology
- Identify possible cortical CMIs – or other lesions of interest – on the acquired images. These lesions are the targets for histological analysis. Watch out for artifacts, such as post-mortem tissue damage (which sometimes appear at the surface of brain slabs due to cuts) or long-term formalin storage artifacts (e.g., coarse MRI hypointensities representing neuropil changes8).
Note: Different histopathological subtypes of cortical CMIs have different MR characteristics. For further details on CMI subtypes, the reader is referred to a recent ex vivo study7. - After identifying possible cortical CMIs on the MR images, sample the region of interest for histopathological validation. Make sure to cut out a region, containing anatomical landmarks, for later matching of the MRI with histopathology. Perform standard histopathology, as followed (but other approaches might also apply).
- Cut out a region of approximately 30 x 20 x 5 mm3 containing a possible cortical CMI.
- To obtain accurate sampling, estimate the lesion location by the slice thickness of the MR images, and tissue architecture. Manually cut the tissue slightly above the estimated lesion location to limit the amount of serial sectioning (after paraffin embedding) that is needed for targeting the lesion.
- Make sure the sampled tissue fits a tissue cassette. Place the surface to be cut face-down in the cassette.
- Keep all tissue cassettes in 10% formalin, until processing of the tissue.
- Process the tissue for paraffin embedding. This usually involves an automated procedure of dehydrating the tissue, through a series of graded alcohol (e.g., 70% to 95% to 100%) baths, and clearing of the tissue in xylene.
- Embed the tissue in paraffin wax blocks. Ensure the surface to be cut faces up after embedding.
- Cut 4-6 µm serial sections with a microtome, until the targeted lesion is retrieved.
- Float the sections on the surface of a 37 °C water bath. Mount the sections on glass slides. Place the slides on a warming block to bond the tissue to the glass. Store slides O/N at RT.
- Perform an appropriate staining (e.g., H&E staining) on the first sections, keep adjacent blank sections for further use (e.g., immunohistochemistry).
- Coverslip the H&E stained sections, using a drop of mounting medium of choice. Gently lower the slip, avoiding air bubbles.
- Study the sections using a light microscope, at an appropriate magnification. Compare sections to the previously obtained MR images.
- Identify possible cortical CMIs – or other lesions of interest – on the acquired images. These lesions are the targets for histological analysis. Watch out for artifacts, such as post-mortem tissue damage (which sometimes appear at the surface of brain slabs due to cuts) or long-term formalin storage artifacts (e.g., coarse MRI hypointensities representing neuropil changes8).
2. Assessing Cortical Microinfarcts on In Vivo 7T MRI
- Perform 7T MRI in the patient population of your interest, using the in vivo MRI protocol (which includes at least a 3D FLAIR) as described in6.
- Assess cortical CMIs on the in vivo 7T MR images as detailed in the steps below, using the following 7T rating criteria for CMIs: cortical CMIs are hyperintense on FLAIR (with or without a hypointense center), hyperintense on T2, hypointense on T1, detectable on at least two views of the brain (e.g., sagittal and transversal), restricted to the cortex, distinct from perivascular spaces, with a greatest dimension ≤4 mm6,7.
- Use an interface with three image viewers, to simultaneously view FLAIR, T1, and T2 images, e.g., MeVisLab (Figure 3). This platform allows to incorporate multiple viewers and to place markers on possible lesion locations.
- First assess one hemisphere on FLAIR in sagittal view. Screen the whole cortex for hyperintense lesions. Any hyperintens lesion ≤4 mm is a possible CMI. Place markers by clicking on each possible CMI.
- Repeat for the other hemisphere.
- Verify all marked locations on T1 and T2. Discard a location if it is not hypointense on T1 or hyperintense on T2.
- Assess transversal view, on FLAIR, T1, and T2. Discard a location if it is not visible. Check the coronal view in case of doubt.
- Watch out for MRI artifacts and anatomical variations (especially sulcal edges).
- Save markers.
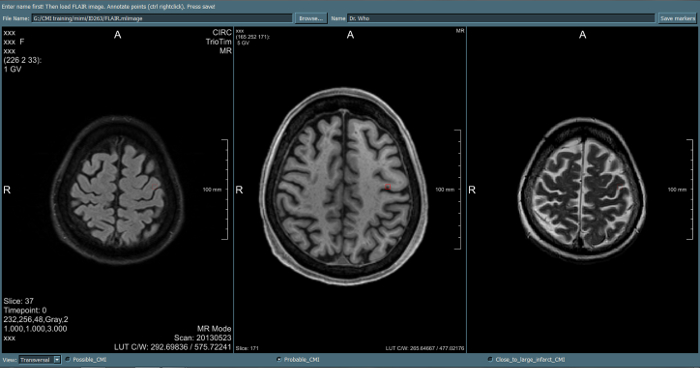
Figure 3. Example image viewing platform for the assessment of cortical microinfarcts. An interface is used, integrated in MeVisLab. This program allows to incorporate multiple viewers simultaneously, to switch easily between sagittal / transversal / coronal orientation, and to place and save markers on possible lesion locations. (Different markers can be chosen for different types of lesions).
3. Assessing Cortical Microinfarcts on In Vivo 3T MRI
- Acquire 3T MR images of the patient population of your interest. Existing data can also be used as long as the MR imaging protocol contained at least a 3D T1, and a FLAIR and T2.
- Assess cortical CMIs on the in vivo 3T MR images as detailed in the steps below, using the following 3T rating criteria for CMIs: cortical CMIs are hypointense on T1 (isointense with CSF), detectable on at least two views of the brain (e.g. sagittal and transversal), restricted to the cortex, distinct from perivascular spaces, with a greatest dimension ≤4 mm.
- Explore the location of a hypointense cortical lesion found on T1 on FLAIR and T2 weighted images. Rate the lesion as a probable cortical CMI if the location is hyperintense or isointense (with the grey matter) on FLAIR and T2. Discard the lesion if at the same location a hypointense signal is found on T2, indicating the T1 hypointense lesion is either due to a hemorrhagic lesion, a vessel, or an artifact. In case of doubt, check the location on a T2* weighted image9.
- Use the same interface as described above.
- First assess one hemisphere on T1 in sagittal view. Screen the whole cortex for focal hypointense lesions. Any hypointense lesion ≤4 mm is a possible CMI. Place markers by clicking on each possible CMI.
- Repeat for the other hemisphere.
- Assess transversal T1, and simultaneously verify all marked locations on transversal FLAIR and T2. Regard the location as a probable CMI if it is hyperintense or isointense on FLAIR and T2. Discard a location if it seems to be an artifact or anatomical variation. Discard a location if it is hypointense on T2.
- Watch out for artifacts that look like CMIs on T1 weighted images, especially ringing artifacts at the ‘edges’ of the brain which will appear at several adjacent gyri, watch out for edges of sulci, watch out for large vessels in the temporal lobes (at the poles). Finally, it is recommended to discard possible cortical CMIs in tissue in close proximity to a larger cortical infarct.
- Save markers.
An impression of the high resolution and high image quality of an ex vivo sequence acquired at 7T is provided here (Figure 4). This is a 3D T2* weighted ex vivo scan, with an isotropic resolution of 0.18 mm. Tissue was derived from an 84-year old demented female with pathologically proven Alzheimer’s disease and severe cerebral amyloid angiopathy (CAA). The detail of the image allows the identification of cortical microvascular pathology. T2* is susceptible for iron, as well as air. This tissue contains a high burden of microvascular pathology within the cortex. The hypointensities in the sulci of these slabs are the results of air bubbles, which can interfere with rating cortical microvascular pathology. For the identification of cortical CMIs, a T2 weighted sequence is required.
Figure 5 represents a cortical CMI identified on ex vivo images at 7T. This cortical CMI was found in the post-mortem brain tissue of an 86-year old female with moderate Alzheimer pathology (Braak & Braak stage IV). The corresponding H&E section verified that this lesion is a chronic gliotic CMI with cavitation7.
Figure 6 is a representative probable cortical microinfarct, detected on in vivo 7T MRI.
Figure 7 is a representative probable cortical microinfarct, detected on in vivo 3T MRI.
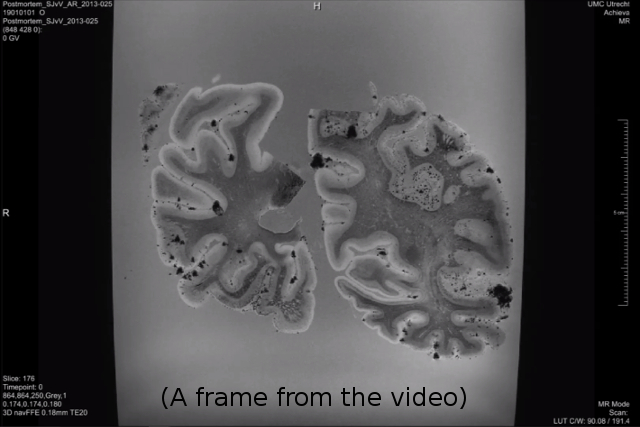
Figure 4. Representative post-mortem images acquired at 7T. Please click here to view this video.
This is a 3D movie of a 0.18 mm isotropic T2* weighted image of a case with severe amyloid angiopathy. These brain slabs have been generously provided by Dr. Annemieke Rozemuller, VUMC, Amsterdam.
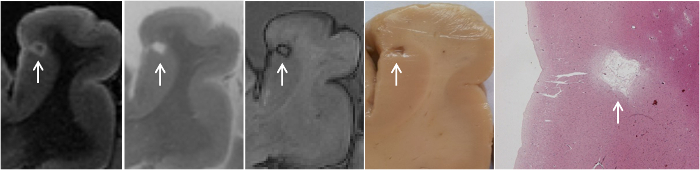
Figure 5. MR-guided histopathology of cortical microinfarct.
Depicted are a FLAIR, T2, T1, wet tissue, and H&E staining, showing a cortical chronic gliotic microinfarct with cavitation. This figure has been modified from7. Please click here to view a larger version of this figure.

Figure 6. Representative probable cortical microinfarct on 7T MRI.
A cortical microinfarct on 7T is hyperintense on FLAIR and T2, and hypointense on T1. This case is a 45-year old female who suffered from a lobar intracerebral hemorrhage. MR images are a courtesy of Dr. Karin Klijn, UMCU, Utrecht. Please click here to view a larger version of this figure.
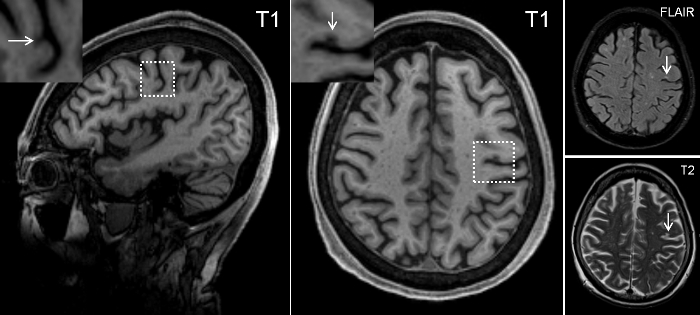
Figure 7. Representative probable cortical microinfarct on 3T MRI.
A cortical microinfarct on 3T can best be identified as a hypointense lesion on a 3D T1. The corresponding location on FLAIR and T2 should be hyperintense (in this case) or isointense. This case is a 76-year old female with a clinical diagnosis of Alzheimer’s disease. MR images are a courtesy of Dr. Christopher Chen, NUS, Singapore. Please click here to view a larger version of this figure.
| TI | TR / TE | Flip / refocusing angle | Acquired resolution | Matrix size | Slices | Averages | Scan duration | |
| (ms) | (ms) | (°) | (µm3) | (h:min:sec) | ||||
| T2 | – | 3,500 / 164 | 90 / 40 | 400x400x400 | 500×280 | 100 | 4 | 1:52:03 |
| FLAIR | 1,600# | 8,000 / 164 | 90 / 40 | 400x400x400 | 500×280 | 100 | 4 | 4:16:08 |
| T1 | 280 | 7.7 / 3.5 | 6 / – | 400x400x400 | 348×348 | 80 | 3 | 0:55:38 |
| T2* | – | 75 / 20 | 25 / – | 180x180x180 | 832×834 | 278 | 1 | 4:59:31 |
| No sensitivity encoding (SENSE) acceleration was applied. # The TI was determined based on 10% formalin. | ||||||||
Table 1. Post-mortem scan parameters.
