The atherosclerotic plaque induction procedure takes 15 – 20 min and shows a minimal mortality rate, mostly due to the bleeding occurring during the procedure. After surgery, the mice recover from anesthesia within 20 – 25 min. No physical impairment, such as paralysis, or feeding disturbance was observed after the surgery.
The wire-injury induces a de-endothelialization, mimicking vascular lesions after balloon denudation or stent-implantation. Immediately after injury, the denuded vascular wall will be covered with a layer of thrombocytes, which mediates and favors the adhesion of the monocytes12. Activated smooth muscle cells from the media will proliferate and migrate into the intimal spaces, forming the neointima. Other progenitors for smooth muscle cells will migrate from the blood (estimated to be 40%) and contribute to the neointima growth. The plaque formation will end after the complete re-endothelialization, usually 4 weeks after the wire-injury.
The neointima formation can be assessed using Movat staining. The plaque size is calculated for each slide using software as shown in Figure 2B. The total plaque size (left carotid artery) can vary between 70,000 – 100,000 µm², while the control vessel size (right carotid artery) can vary between 7,000 – 8,000 µm². These values depend largely on the surgeon. Therefore, we strongly recommend using the same surgeon during the experiments for the same study.
The developed plaque resembles in stent restenosis, which predominately consists of proliferated and migrated smooth muscle cells from the media. The cellular composition determined by immunological staining procedures shows that the smooth muscle cell content is approximately 30 – 40%, while macrophages are found in 15 – 25% of the neointima of the injured vessel. The re-endothelialization can be measured after staining for an endothelial marker, and calculated as the percentage of circumference stained over the entire circumference of the lumen. Usually the re-endothelialization reaches 80 – 90% after 3 weeks, and should almost be complete after 4 weeks (Figure 2C). To track the plaque growth during its development, the same analysis can be repeated for every time-point after the wire-injury, depending on the interest and the subject studied (see Table 1).
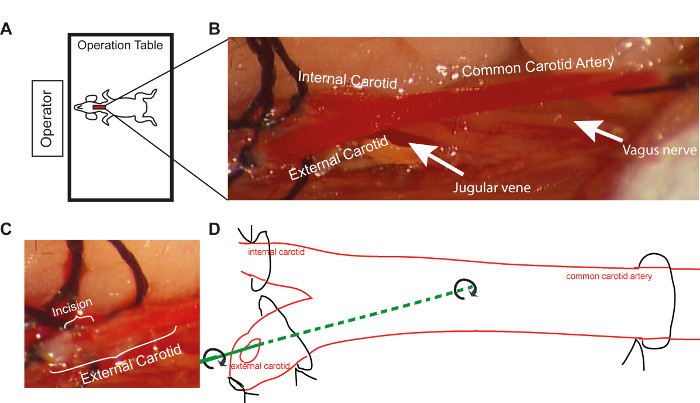
Figure 1. Schematic Representation of Operative Procedure. (A) The positioning of the operation table toward the operator during the wire-injury procedure (B) Enlarged view of the common carotid artery and its branches, as it appears under the microscope at 10X magnification (C) The size of the incision in the external carotid artery under the microscope at 10X magnification (D) Schematic representation of wire-injury procedure using the 14 inch guide wire. Please click here to view a larger version of this figure.
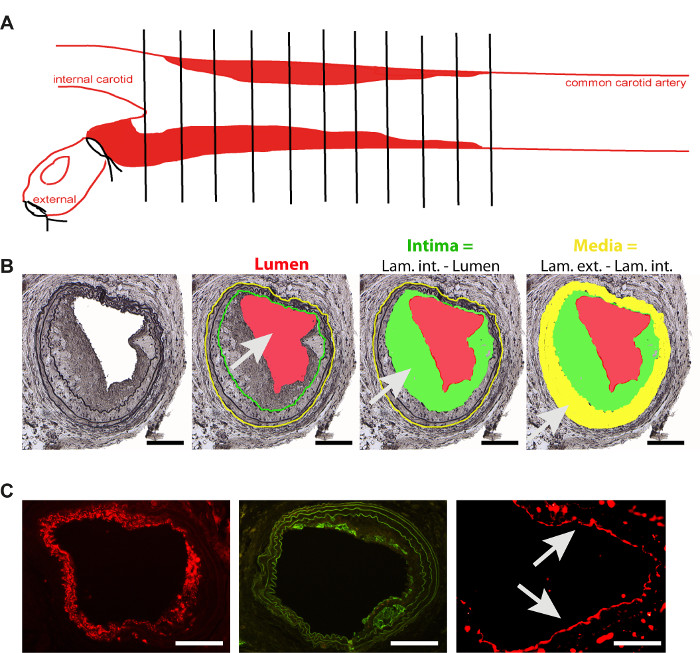
Figure 2. Analysis of Restenosis Plaque. (A) Schematic representation of plaque analysis in the common carotid artery, 4 weeks after wire-injury induction (B) Neointima formation 4 weeks after the wire-injury and schematic representation of main parameters used for analysis. Intima (green area) is the difference between the lumen (red) and the lamina interna (green line). Media (yellow area) is the difference between the lamina externa (yellow line) and interna (green line). Scale bar 100 µm (C) Representative images of the staining of the main cell types involved in neointima formation. Smooth muscle cells (smooth muscle actin -red, scale bar 100 µm), macrophages (Mac 2- green, scale bar 100 µm) and endothelial cells (CD31- red, arrows, scale bar 50 µm). Please click here to view a larger version of this figure.
| Time | Trombus | Plaque (µm²) | Macrophages (% from Plaque) |
Smooth muscle cells (% from Plaque) |
Re-endothelialization (% lumen circumference) |
| 1 day | present | 0 | 0 | 0 | 0 |
| 1 week | – | < 30 000 | > 10 | < 50 | < 50 |
| 2 weeks | – | < 50 000 | > 10 | < 50 | > 50 |
| 3 weeks | – | < 70 000 | 15-25 | 30-40 | 80-90 |
| 4 weeks | – | 70 000 – 100 000 | 15-25 | 30-40 | complete |
Table 1. Time-dependent Plaque's Development.
| Model | Animals | Advantages | Disanvantages |
| Diet-induced native atherosclerosis | Small |
|
|
| Big |
|
|
|
| Balloon dilatation | Small |
|
|
| Big |
|
|
|
| Wire Injury | Small |
|
|
| Stent implantation | Small |
|
|
| Big |
|
|
Table 2. Advantages and Disadvantages of Existent Models of Arterial Injury.
