Murine bone marrow derived macrophages can be cultured from hematopoietic cell precursors in bone marrow aspirates. Bone marrow aspirates pooled from femurs and tibias of one C57BL/6 mouse typically yield 107 bone marrow derived macrophages, making them a convenient source of macrophages for experiments. BMDMs can be used to test antibody based drug responses when challenged with an inflammatory stimulus in vitro. Figure 1 shows that IVIg brand, Gammunex (GX), + LPS increases the production of the anti-inflammatory cytokine, IL-10, 7-fold compared to LPS stimulation alone (Figure 1A) and decreases the production of IL-12/23p40 (Figure 1B). Figure 1 also demonstrates that different IVIg preparations perform differently. Although the three different preparations of IVIg are able to decrease IL-12/23p40 significantly (Figure 1B), Octagam (OG) and Gammagard liquid (GL), do not significantly increase IL-10 production in response to LPS (Figure 1A). OG and GL are able to significantly reduce IL-12/23p40 production in response to LPS, but to a lesser degree than GX. These results demonstrate that antibody affects bone marrow derived macrophage activation, and that there are differences between preparations of the same drug that can cause changes in responses.
BMDMs can be used to test the mechanistic effects of IVIg, by western blotting. Macrophages activated with IC + LPS have increased phosphorylation of the mitogen activated protein (MAP) kinases, p38 and Erk1/2, which are responsible for increased IL-10 production21. Results in Figure 2 show a typical western blot to detect MAP kinase activation required for IL-10 production by macrophages that are unstimulated, or have been stimulated with LPS, IVIg, or IVIg + LPS. IVIg stimulation alone or IVIg + LPS co-stimulation increased activation of the MAP kinases, Erk1/2, with earlier and prolonged phosphorylation compared to that seen with LPS alone. Activation of p38 occurred earlier in macrophages stimulated with IVIg + LPS compared to those stimulated with LPS alone. These results show that methods, such as western blotting, can be used to show cell signaling effects of antibody drugs on BMDMs. In addition to cytokine production, MAP kinase activation can be used to show that anti-inflammatory macrophage activation has occurred.
Mature, tissue resident macrophages can also be isolated from mice to assess responses to IVIg 5.0 x 105 – 1.0 x 106 peritoneal macrophages can be isolated from one healthy C57BL/6 mouse. In Figure 3, peritoneal macrophages from mice injected with IVIg do not significantly increase IL-10 production in the absence of stimulation in vitro, compared to PBS injected mice. When peritoneal macrophages from IVIg injected mice are stimulated with LPS ex vivo, they produce 6-fold more IL-10 than mice injected with PBS. They do not, however, produce detectable amounts of IL-12/23p40 when stimulated with LPS ex vivo. These results demonstrate that antibody effects can be tested on macrophages by injecting the drug in vivo and culturing cells ex vivo with this method.
Macrophage responses to antibodies and inflammatory stimuli can be assessed in vivo. Cytokine production can be assessed in lavage fluid, and in supernatants from ex vivo stimulated peritoneal macrophages. Figure 4 shows the anti-inflammatory cytokine IL-10 is increased in lavage fluid (Figure 4A), peritoneal cells (Figure 4B), and peritoneal macrophages (Figure 4C) when mice are challenged with IVIg + LPS compared to PBS + LPS. Production of the pro-inflammatory cytokine subunit, IL-12/23p40, is significantly reduced in cultured peritoneal macrophages, but not in lavage fluid. This method allows examination of an antibody drug's impact on inflammatory responses in vivo as well as ex vivo.
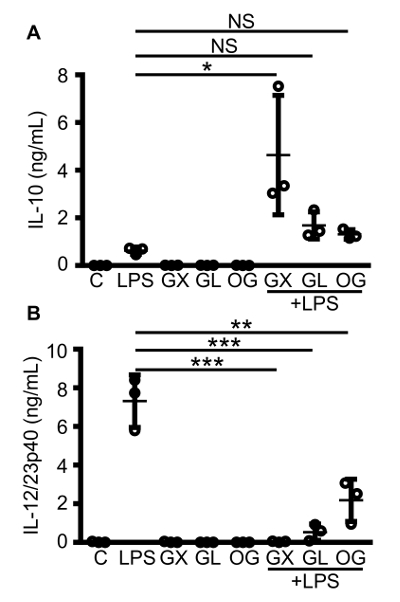
Figure 1: Macrophage IL-10 and IL-12/23p40 production in response to co-stimulation with different brands of IVIg and LPS. C57BL/6 MCSF bone marrow derived macrophages were either unstimulated (C), or stimulated with LPS (10 ng/mL), IVIg (30 mg/mL), or IVIg + LPS. Three different brands of IVIg were tested: Gammunex (GX), Gammagard liquid (GL), and Octagam (OG). Macrophage supernatants were collected 24 h after stimulation, and clarified by centrifugation. ELISAs for IL-10 (A) and IL-12/23p40 (B) were performed. Data are for macrophages from n = 3 independent experiments, with cells from 1 individual mouse per experiment, with ELISAs assayed in duplicate. Data are means ± SD. *P <0.05, ** P <0.001, ***P <0.0001 for comparison between LPS stimulation and IVIg + LPS co-stimulation. One-way analysis of variance (ANOVA) with Tukey's post-test for multiple comparisons were used for statistical analyses. Please click here to view a larger version of this figure.
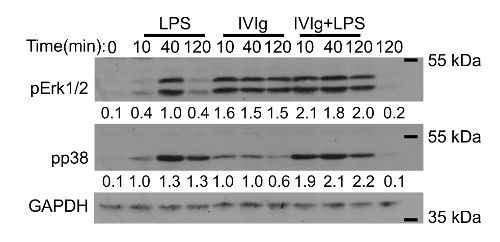
Figure 2: Western blot analysis of MAP kinase activation in IVIg-activated macrophages. MCSF derived bone marrow macrophages were unstimulated or stimulated with LPS (10 ng/mL), GX IVIg (30 mg/mL), or GX IVIg + LPS; for 0, 10, 40, or 120 min. Whole cell lysates (1.0 x 106 macrophages/lane) were subjected to sodium dodecyl sulfate-polyacrylamide gel electrophoresis (SDS-PAGE) and western blotting with phospho-specific antibodies for p38 and extracellular signal-regulated kinase (Erk1/2), as well as glyceraldehyde 3-phosphate dehydrogenase (GAPDH), as a loading control. Results shown are representative of n = 3 independent experiments, with cells from 1 individual mouse per experiment. Densitometry for pp38 and pErk1/2 protein levels, normalized to GAPDH, averaged from 3 independent experiments are shown below each band. This figure has been modified from Kozicky et al8. Please click here to view a larger version of this figure.
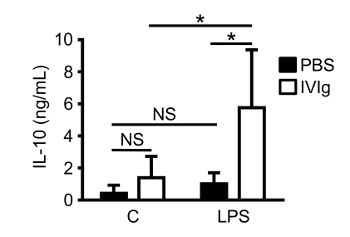
Figure 3: IL-10 production by macrophages from mice challenged with IVIg in vivo. 8-week-old C57BL/6 mice were given sterile PBS (injection control) or GX IVIg (2.5 g/kg) intraperitoneally. After 1 h, mice were euthanized and peritoneal lavages were performed. Peritoneal macrophages were isolated using adherence selection. Macrophages were either unstimulated (C), or stimulated with LPS (10 ng/mL). Cell supernatants were harvested and clarified after 24 h for IL-10 ELISAs. Data are from n = 5 individual mice per group performed in 3 independent experiments, with ELISAs assayed in duplicate. Data are means ± SD. * P <0.01 and NS = not significant. Statistical analyses were performed using a Two-way ANOVA with Sidak's posttest for multiple comparisons. This figure has been modified from Kozicky et al8. Please click here to view a larger version of this figure.
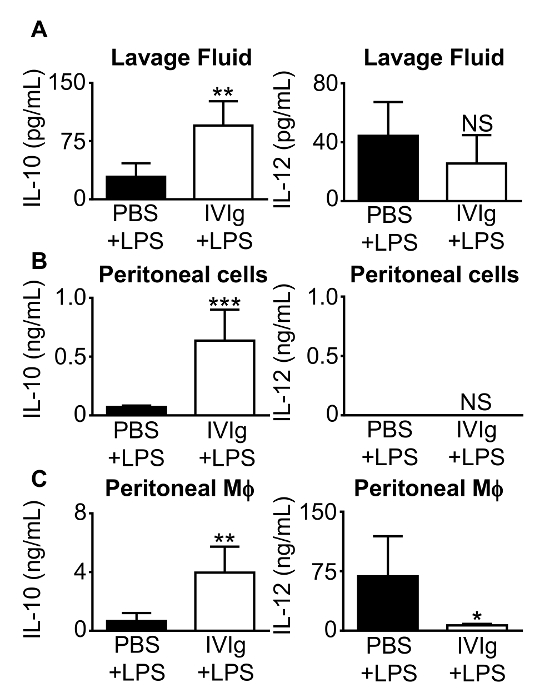
Figure 4: IL-10 and IL-12/23p40 production from mice challenged with IVIg + LPS in vivo. 8-week-old C57BL/6 mice were injected intraperitoneally with either PBS + LPS (0.2 µg/g body weight), as a control; or GX IVIg (2.5 g/kg body weight) + LPS (0.2 µg/g body weight). After 1 h, mice were euthanized and peritoneal lavages were performed. (A) Clarified lavage fluid, (B) clarified conditioned supernatants from peritoneal cells during a 1 h macrophage adherence step, and (C) clarified 24 h peritoneal macrophage (Mφ) supernatants were assayed for IL-10 and IL-12/23p40 by ELISA. Data are means ± SD for n = 5 mice in 3 independent experiments, with ELISAs assayed in duplicate. *P <0.05, **P <0.01, ***P <0.001, and NS = not significant. Mice injected with PBS + LPS were compared to mice injected with IVIg + LPS using a Student's t test. This figure has been modified from Kozicky et al8. Please click here to view a larger version of this figure.
