A total of 34 rats were randomly divided into the following groups: Sham (n = 17), Excision (n = 17), and Nerve Graft (n = 10) for the operation. All rats survived surgery and the postoperative period uneventfully. One week after surgery and for the subsequent 100 days, all animals underwent the functional tests described above once a week. The representative results of each of these tests are described below.
Grasping Test
The percentage of rats with a positive response in the grasping test was highest for the Sham group. This value gradually increased over time in rats from the Crush and Nerve Graft groups (Figure 3).
Pin Prick Test
Rats from the Sham group had the best scores in the cumulative pin prick test relative to rats from the Nerve Graft group. Both had better scores than the rats in the Excision group (Figure 4).
Ladder Running Test
The rats’ velocity in the ladder running test was highest in the Sham group than in the rats submitted to MN lesion. Among the latter, the time to run the ladder tended to decrease over time, paralleling MN recovery (Figure 5).
Rope Test
As in the ladder running test, the time the rats took to climb the rope was shorter in the Sham group compared to the groups in which the MN was injured. The rats' speed in this test increased when the MN was allowed to recover (Figure 6).
Walking Track Analysis
Analysis of walking tracks tended to show changes in the morphology of paw prints (Figure 7). These changes were often more pronounced in crushing injuries than in segmental nerve lesions50.
Infrared Thermography
Thermography was useful when examining temperature differences between the forepaws in the first 30 days after surgery. Temperature differences were more noticeable in rats with a more severely injured MN, such as in those from the Excision group (Figure 8 and Figure 9).
Electroneuromyography
Table 1 summarizes the biological importance of the electroneuromyography measurements, providing representative results for the different experimental groups. Various patterns were observed with electroneuromyography. A normal CMAP was typical of a rat from the Sham group, while a polyphasic CMAP was associated with a variable degree of lesion of the MN, as in the Crush and in the Nerve Graft groups (Figure 10). In the Excision group, no CMAPs were observed.
Wrist Flexion Strength
Given that wrist flexion is mainly dependent on the MN, this test was used to evaluate motor recovery in this nerve’s territory. Wrist flexion strength was closest to normal when recovery was maximal (Figure 11).
Muscle Weight and Morphology
The weight and morphology of the flexor carpis radialis muscle were dependent on MN recovery, as this muscle is innervated exclusively by the MN9,10. Thus, normal weight and morphology were observed in the Sham group. A loss of weight and muscle trophism was observed in the Crush, Nerve Graft, and Excision groups (Figure 12).

Figure 1: Schematic representation of the anatomy of the median nerve of the rat.
(1) Origin and termination of the median nerve in the rat brain (green area = primary motor area; blue area = primary sensory area). (2) Transverse section of the spinal cord at C7 segment level; (3) Axillary nerve; (4) Musculocutaneous nerve; (5) Radial nerve; (6) Median nerve; (7) Ulnar nerve; (8) Medial cutaneous branch of the arm; (9) Medial cutaneous branch of the forearm; (10) Axillary artery; (11) Brachial artery; (12) Median artery; (13) Superficial radial artery; (14) Ulnar artery; (15) Motor branch of the median nerve to the pronator teres muscle; (16) Motor branch of the median nerve to the flexor carpis radialis muscle; (17) Motor branch of the median nerve to the flexor digitorum superficialis muscle; (18) Motor branch of the median nerve to the flexor digitorum profundus muscle; (19) Sensory branch of the median nerve to the thenar region; (20) Common palmar artery of the first interosseous space; (21) Radial palmar digital artery of the first digit; (22) Motor branch of the median nerve to the thenar muscles; (23) Palmar arterial arch; (24) Radial palmar digital nerve of the first digit; (25) Ulnar palmar digital nerve of the first digit; (26) Common palmar artery of the third interosseous space; (27) Motor branches of the terminal divisions of the median nerve to the first three lumbrical muscles; (28) Ulnar palmar digital nerves of the second, third, and fourth digits; (29) Ulnar palmar digital arteries to the fourth and fifth digits; (30) Radial palmar digital nerves of the second, third, and fourth digits; (31) Radial palmar digital artery of the fifth digit; (32) Skin territory of the median nerve in the forepaw (blue-shaded region). Please click here to view a larger version of this figure.
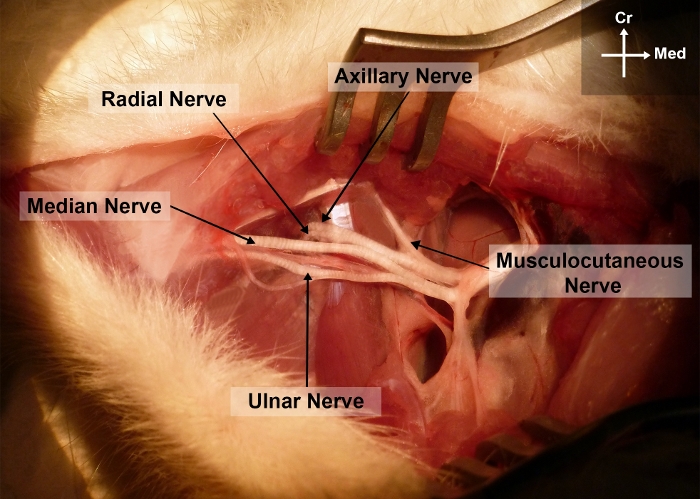
Figure 2: Photograph of the right forelimb of the rat showing the surgical anatomy of the median nerve in the arm and axillary regions.
Cr, cranial; Me, medial Please click here to view a larger version of this figure.
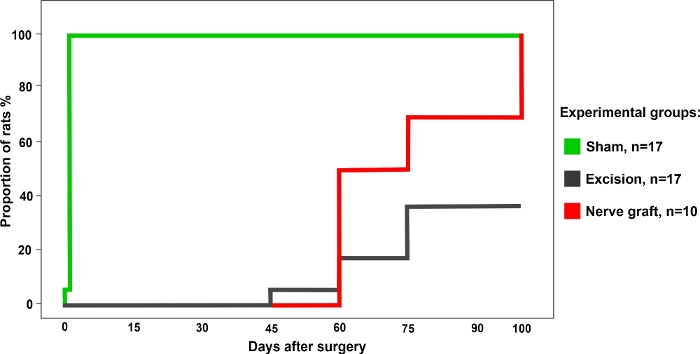
Figure 3: Percentage of rats with a positive grasping test in the different experimental group over a period of 100 days after surgery. Please click here to view a larger version of this figure.
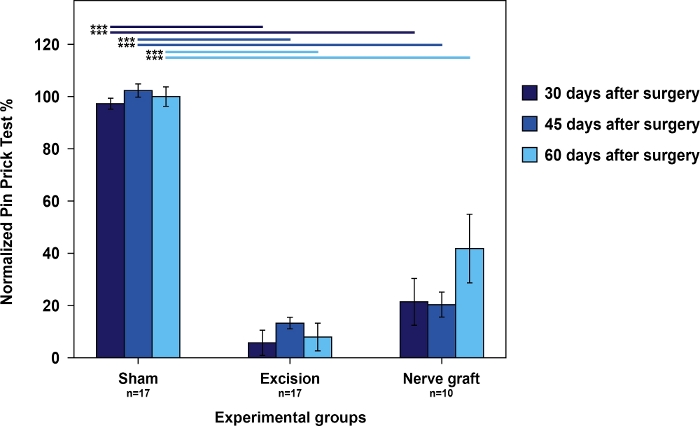
Figure 4: Nociception evaluation using cumulative pin prick test results in the operated forepaw normalized to the contralateral paw in the different experimental groups.
Vertical bars represent 95% confidence intervals. Horizontal lines in the upper part of the figure indicate statistically significant differences between experimental groups, ***p<0.001. Please click here to view a larger version of this figure.

Figure 5: Average speed in the ladder running test in the different experimental groups.
Vertical bars represent 95% confidence intervals. Asterisks in the upper portion of the figure indicate statistically significant differences between groups, *p<0.001. Please click here to view a larger version of this figure.
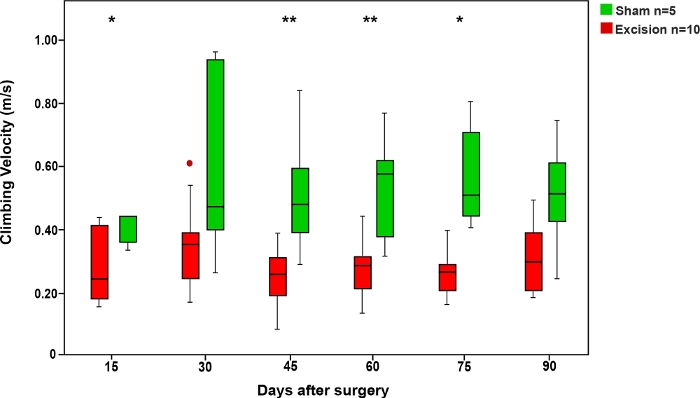
Figure 6: Average climbing velocity in the rope test in the Sham and Excision groups.
Vertical bars represent 95% confidence intervals. Asterisks in the upper portion of the figure show statistically significant differences between groups, *p<0.05; **p<0.01. Please click here to view a larger version of this figure.
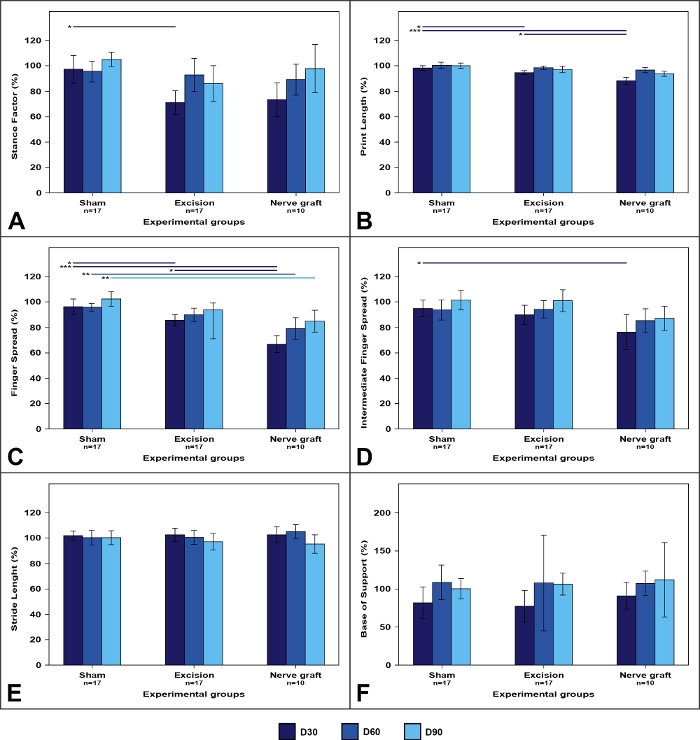
Figure 7: Walking track parameters in the different experimental groups.
Values on the operated limb are expressed as percentages of means normalized to the contralateral limb. (A) Stance factor; (B) Print length; (C) Finger spread factor; (D) Intermediate finger spread factor; (E) Stride length; (F) Base of support. Vertical bars represent 95% confidence intervals. Horizontal lines in the upper portion of the figure indicate statistically significant differences between experimental groups. D30, D60, D90 = 30, 60, and 90 days after surgery, *p<0.05; **p<0.01; ***p<0.001. Please click here to view a larger version of this figure.
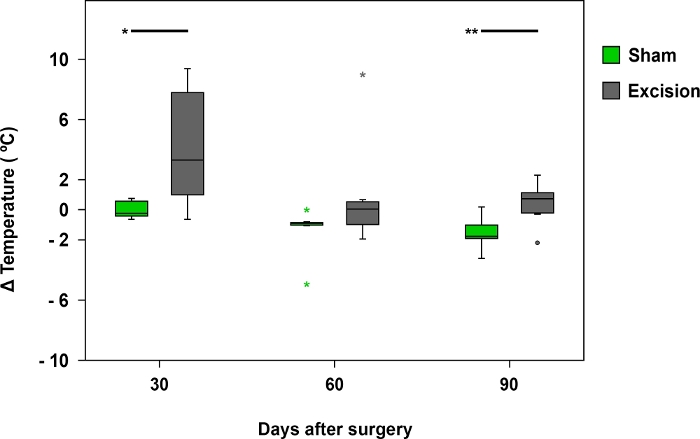
Figure 8: Mean temperature difference registered by infrared thermography.
The box plots represent the temperature difference between the palmar region of the median nerve on the operated side (right side) and the contralateral side (left) in the Sham (n = 17) and Excision (n = 17) groups, *p<0.05; **p<0.01. Please click here to view a larger version of this figure.
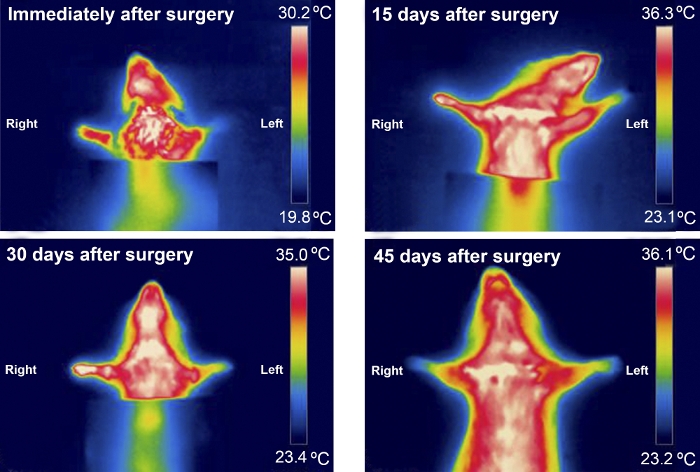
Figure 9: Typical infrared thermography pattern of an animal from the excision group during the first 45 days after surgery. Please click here to view a larger version of this figure.

Figure 10: Typical patterns of Compound Muscle Action Potentials (CMAPs) from an animal from the Sham and Nerve Graft groups 90 days after surgery. Please click here to view a larger version of this figure.
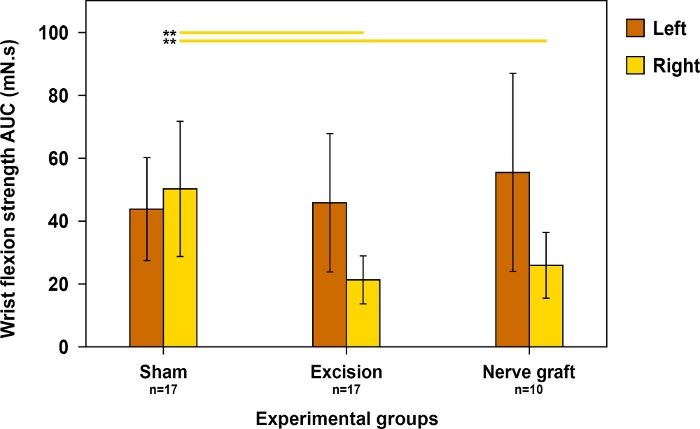
Figure 11: Evaluation of wrist flexion strength on both forepaws 90 days postoperatively in different experimental groups.
Wrist flexion strength was assessed using the area under the curve (AUC) over a time period of 30 s and using supratetanic stimulation. Vertical lines denote 95% confidence intervals. Horizontal lines in the upper portion of the figure highlight statistically significant differences between groups, **p<0.01. Please click here to view a larger version of this figure.
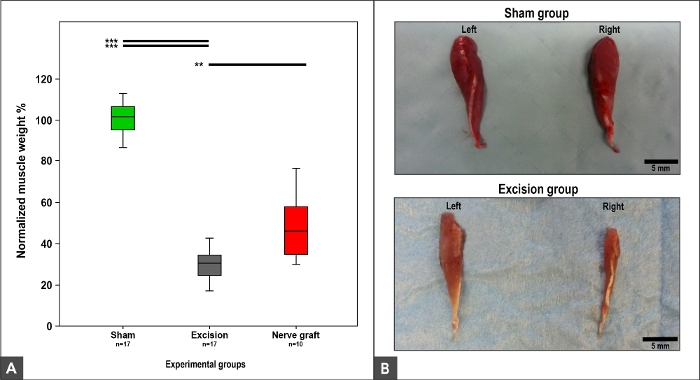
Figure 12: Flexor carpi radialis muscle weight and macroscopic appearance 100 days after surgery.
(A) Box plots depicting the normalized flexor carpi radialis muscle weight in different experimental groups, **p<0.01; ***p<0.001. (B) Photographs of the muscles on the right and left sides in the Sham and Excision experimental groups. Please click here to view a larger version of this figure.
| Parameter | Parameter significance | Sham group | Excision group | NG group |
| Neurological stimulation threshold (%) | Evaluation of nerve regeneration, as there is a minimal number of nerve fibers required to produce either a CMAP or a visible muscle contraction12 | 281.63 ± 271.65 | 5359.98 ± 3466.52 | 2108.12 ± 2115.13 |
| Motor stimulation threshold (%) | Evaluation of nerve regeneration, as there is a minimal number of nerve fibers required to produce either a CMAP or a visible muscle contraction12 | 462.52 ± 118.91 | 1694.10 ± 503.24 | 1249.50 ± 503.24 |
| Latency (%) | Assessment of nerve conduction velocity in the fastest nerve fibers, that is to say the largest myelinated fibers44 | 113.55 ± 25.04 | N/A | 132.80 ± 69.95 |
| Neuromuscular transduction velocity (%) | Assessment of nerve conduction velocity in the fastest nerve fibers, that is to say the largest myelinated fibers44 | 92.01 ± 20.88 | N/A | 91.30 ± 26.51 |
| CMAPs amplitude (%) | Evaluation of the number of reinnervated motor units34 | 110.63 ±45.66 | N/A | 41.60 ± 24.84 |
| CMAPs duration (%) | Assessment of synchrony of muscle innervation, which is dependent on the degree of muscle reinnervation and myelination of the innervating motor fibers44,45 | 101.12 ± 23.92 | N/A | 151.06 ± 54.52 |
| NG, nerve graft CMAPs, compound muscle action potential. N/A, non-applicable All parameters are expressed as percentages of the average contralateral values. Numeric variables are expressed as average ± standard deviation. |
||||
Table 1: Electroneuromyographic assessment at the end of the experiment.
