All animal experiments require approval by ethical authorities.
1. Mouse Sacrifice and Microdissection of Aorta
- Sacrifice the mouse by CO2 asphyxiation and record weight.
- Spray the mouse with 70% ethanol to avoid fur contamination of the samples. Place the mouse in a supine position. From the jugular notch, make a midline incision using Mayo scissors extending it almost down to the pubic bone.
CAUTION: High percentage ethanol is highly flammable and could cause serious eye irritation. Take precautionary measures. - Use a 23 G needle to exsanguinate the mouse by cardiac puncture through the thorax wall. This procedure usually yields 750 µL of blood from a 20 week old mouse. Typically, collect half of the volume in a tri-potassium EDTA-coated tube and the other half in a serum or lithium heparin-coated tube. Gently turn the tubes and keep them at room temperature until further processing.
- Use Mayo scissors to cut the parietal peritoneum in the midline to open the abdominal cavity. Hold the xiphoid process with tissue forceps and cut open the peritoneum laterally on both sides and continue to open the diaphragm.
- Use the Mayo scissors to open the chest cavity by cutting through the rib cage as laterally as possible. This will enable wide angles for the instruments while microdissecting the aorta later on.
- Make an incision in the right auricle for perfusion fluid drainage. Insert a 27 G needle through the apex of the heart in cranial direction. Keep the needle fixed in the left ventricle while slowly perfusing the mouse with 10 mL ice-cold phosphate-buffered saline (PBS) during minimum 2 min. Observe the liver shifting in color and getting paler.
NOTE: Some protocols use paraformaldehyde perfusion, but this interferes with several downstream applications, such as immunohistochemistry analysis of lymphocytes. Therefore, no perfusion fixation with paraformaldehyde is performed in this protocol. - Dissect organs of interest (e.g. lymph nodes, spleen, liver, intestine, inguinal fat pads, kidneys, etc.) using anatomical forceps and dissecting scissors.
- Cut trachea and esophagus on the right side of the heart without damaging the aortic arch. Cut the diaphragm and structures attaching the viscera to retroperitoneum, leaving the heart, aorta, and kidneys in situ. Fold away the lungs and viscera caudally and cover them with a napkin to begin retroperitoneal microdissection of para-aortic lymph nodes and abdominal aorta.
- Start microdissection under a stereomicroscope at 6x magnification. Begin to dissect the aortic bifurcation by lifting surrounding tissue with Dumont forceps and cutting under tension with Vannas scissors.
- Continue dissection of the abdominal aorta cranially. Cut abdominal branches from the aorta and free the aorta proximally through the aortic hiatus in the diaphragm.
NOTE: Microdissection requires accurate hand-eye coordination through the stereomicroscope, which takes some practice to master.
- Continue dissection of the abdominal aorta cranially. Cut abdominal branches from the aorta and free the aorta proximally through the aortic hiatus in the diaphragm.
- Remove the adipose tissue covering the thoracic aorta. Carefully dissect dorsally of the thymus to free the aortic arch with branches. Continue dissecting the carotid arteries as distally as possible in the thoracic cavity. In special cases, neck dissection could be performed to include the carotid bifurcation.
- Clean the instruments by consecutive rinses in deionized water, RNase decontamination solution, 70% ethanol, and PBS before actually cutting the aorta. Lift the heart by the apex with the forceps. Cut the aorta close to the heart and place the whole heart in a tube with PBS. The heart could be stored on ice for a couple of hours before continued processing and cryomounting the aortic root.
- Cut the aortic arch according to Figure 1A. Put the aortic arch in a tube containing 1 mL of 4% formaldehyde overnight at 4 °C. The specimen could be stored in this manner for several years before pinning and analysis.
CAUTION: Formaldehyde may cause cancer, allergic skin reactions, and is harmful if swallowed. Use personal protective equipment as required. - Dissect the remaining descending aorta and put it in an RNA stabilization solution or snap freeze it for subsequent RNA analysis or other application. Optimizing work flow to minimize dissection time is crucial to avoid excessive RNA degradation.
- Put the blood collection tubes (collected in step 1.3) in a centrifuge. Spin down the separate plasma and serum tubes at 1,500 x g for 15 min at room temperature. Carefully transfer the plasma and serum to microcentrifuge tubes and store at -80 °C. Collecting both EDTA and heparinized plasma or serum leaves possibilities for multiple downstream applications.
- Place the heart on a cork bed with the ventral side facing up. Fix the heart to the cork with a needle through the apex. Hold the base of the heart with anatomical forceps.
- Use a scalpel to cut away the apical 2/3 of the heart with the direction of the cut being as a line between the two auricles with the scalpel angled 20° caudally in the sagittal plane and 20° cranially in the transversal plane (Figure 1B).
- Embed the aortic root in optimum cutting temperature (OCT) compound, which surrounds, but do not infiltrate the tissue. Immerse the base of the heart in OCT compound. Gently squeeze the heart with the forceps to fill the aortic root with OCT and remove any air bubbles.
- Transfer the specimen to the bottom of a cryomold filled with OCT. The aortic root should now be perpendicular to the bottom surface. Put the mounted heart on dry ice to freeze. Store the specimens in zip lock bags in -80 °C until pursuing cryosectioning according to section 3 in this protocol.
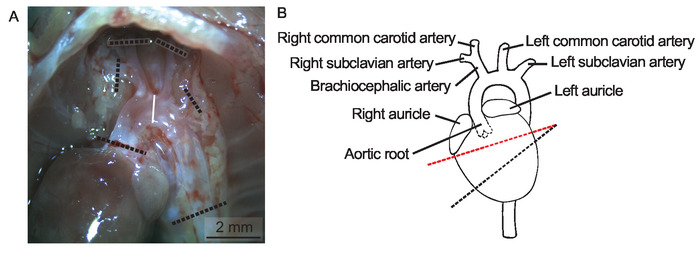
Figure 1: Heart and aortic arch in situ. (A) Lungs, trachea, esophagus, and thymus are removed to display the aortic arch in situ in a 20 weeks old female Apoe-/- mouse on regular chow diet in a micrograph, Scale bar = 2 mm. The dotted lines indicate where to cut the aortic arch and its branches. (B) A schematic depiction of the heart and aorta. The dotted line in red indicates where to cut the heart before cryomounting the aortic root. Please click here to view a larger version of this figure.
2. En Face Analysis of Aortic Arch and Brachiocephalic Artery
- Prepare pinning beds for en face analysis of aortic arches. Fold a segment of paraffin wax film eight times to make a flat 25 mm x 25 mm surface. Wrap it with black electric insulation tape to make a dark background for the aorta. Place a label on the backside of the pinning bed and use a lead pencil to write the mouse identification number (normal pen ink will disappear in the staining process).
- Transfer the aortic arch to the pinning bed and place a drop of PBS on top of it. Begin cleaning the aorta from remaining periadventitial adipose tissue under a stereomicroscope.
- Use Vannas scissors and Dumont forceps to gently peel away all surrounding adipose tissue without manipulating or damaging the aorta. The Sudan IV will stain adipose tissue brightly and it is crucial to remove all such tissue at this point.
NOTE: Keep the aorta moist at all times applying additional PBS when needed.
- Use Vannas scissors and Dumont forceps to gently peel away all surrounding adipose tissue without manipulating or damaging the aorta. The Sudan IV will stain adipose tissue brightly and it is crucial to remove all such tissue at this point.
- Cut open the aorta in the coronal plane by introducing the Vannas scissors in the aortic lumen to expose the intimal surface. Begin to cut the outer curvature of the ascending arch in distal direction and continue to cut open the branches including the brachiocephalic artery. Spare the dorsal part of the descending thoracic region.
- Cut open the lesser curvature and fold open the aorta to display the intimal surface.
NOTE: This step requires fine motor skills and needs some practice to master.
- Cut open the lesser curvature and fold open the aorta to display the intimal surface.
- Pin the open arch to the pinning bed using the blunt end of minutien insect pins. Use a micro Castroviejo needle holder to put the pins in place. Gently bend the pins away from the specimen when in place. Pin the aorta flat on the bed without stretching the specimen. Store the pinned arch facing downwards in a Petri dish filled with PBS at 4 °C.
NOTE: The protocol can be paused here. - Prepare a working solution of Sudan IV. Mix 1 g of Sudan IV powder, 100 mL of 70% ethanol, and 100 mL of acetone in a dark bottle and gently stir for 10 min. There is no need to filter the solution and it can be used for a couple of months if kept dark at room temperature. If the staining color is not satisfactory, a new solution can be made and the specimens stained again.
CAUTION: Acetone is a flammable liquid that could cause serious eye irritation. Store in a well-ventilated place and take precautionary measures when handling. - Arrange five Petri dishes on the lab bench: one filled with 70% ethanol, one filled with Sudan IV working solution, two filled with 80% ethanol, and one filled with PBS.
- Start with rinsing the specimen in 70% ethanol for 5 min by placing the pinning bed in the first Petri dish with the arch facing downwards. Transfer the specimen to the Sudan IV working solution and let it stain the arch for 7 min.
- Next, rinse in 80% ethanol for 3 min twice to destain the normal intimal surface. Destaining time could be adjusted to optimize results. Lastly, rinse in PBS before putting the specimen back into the original Petri dish.
- Acquire micrographs using a stereomicroscope at 10 times magnification connected to a digital camera. Take pictures of the pinned arch submerged in PBS using small metal weights (20 mm x 10 mm x 5 mm) to hold the pinning bed to the bottom of a Petri dish. Place a ruler next to the aorta for calibration of the image.
- Use an image analysis software (e.g. ImageJ) to determine lesion area and total intimal surface. In lack of anatomical landmarks to define the aortic arch, measurement is usually performed from the start of the ascending aorta down to the first intercostal branch (Figure 2A). Use the area quantification feature in the software to manually encircle the total intimal arch area.
NOTE: The lesion quantification should be done in a blinded fashion and it is advisable that a second investigator confirms the results.- In ImageJ, select the polygon selection tool and encircle the total arch area by repetitive clicks. Then select measure in the analyze menu to display the total arch area in the result window.
- Next, encircle all Sudan IV-stained plaques in the arch. Sudan IV is a lysochrome diazo dye that stains lipids, triglycerides, and lipoproteins with an orange-red color. In ImageJ, select the freehand selection tool and encircle all plaques while pressing the Alt key. Click measure in the analyze menu to display lesion-free arch area in the result window.
- Calculate relative lesion area by subtracting the lesion-free area from the total arch area and then dividing the result with the total arch area.
- Carefully pin the subclavian and carotid arteries to enable lesion quantification in the brachiocephalic artery (Figure 2A). Quantification of lesions in the subclavian arteries and the common carotid arteries is usually very challenging and not meaningful, respectively.
- In ImageJ, encircle both pieces of the braciocephalic artery using the polygon selection tool while pressing the shift key. Click measure in the analyze menu to display the total brachiocephalic artery area in the result window.
- Next, select the freehand selection tool and encircle all plaques in brachiocephalic artery while pressing the Alt key. Click measure in the analyze menu to display the lesion-free brachiocephalic artery area in the result window.
- Calculate relative lesion area by subtracting the lesion-free area from the total brachiocephalic artery area and then dividing the result with the total brachiocephalic artery area.
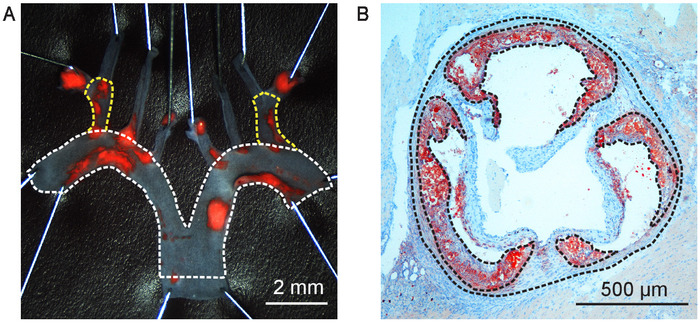
Figure 2: Atherosclerotic lesion quantification. (A) Aortic arch from a 20 weeks old male human APOB100-transgenic Ldlr-/- (HuBL) mouse fed Western diet for ten weeks pinned open and stained for lipid-rich plaques with Sudan IV. Total aortic arch surface area is outlined with the dotted line in white in the micrograph, Scale bar = 2 mm. The dotted lines in yellow outline the total surface area of the brachiocephalic artery. (B) Aortic root cross-section at 400 µm from the aortic sinus in a 20 weeks old male Ldlr-/- mouse fed Western diet for eight weeks visualized in a micrograph, Scale Bar = 500 µm. The dotted lines in black outline the total vessel area and atherosclerotic lesions stained with Oil Red O localized in the arterial intima. Please click here to view a larger version of this figure.
3. Cryosectioning of the Aortic Root
- Set the cryostat temperature at -20 °C and section thickness to 10 µm. Mount the OCT block containing the aortic root on the specimen holder with the ventricular tissue facing outward. While starting to cut, fine tune the alignment of the section surface to be parallel to the specimen holder.
- Remove excessive surrounding OCT to make it easier to collect sections without folds. The aortic root should now be positioned perpendicular to the knife blade given that the base of the heart was placed correctly in the mold.
- Collect initial control sections on ordinary microscope slides, which will be discarded. The first sections should only contain heart muscle tissue. Progress the sectioning by 200 µm at the time. Collect a section and check the progress with a light microscope.
- When getting closer to the left ventricle outflow tract, check every 100 µm under the microscope. When initial indications of a vessel wall are observed, slow down the pace to 50 µm.
NOTE: When the first aortic cusp appears, this will be point zero for collecting sections. It can be difficult to see when the cusps appear exactly, but an exact localization is crucial to perform comparisons of lesions in the same region. - Tilt the specimen towards the point zero cusp to align the section plane with the two other cusps. This is crucial for obtaining true cross sections of the aorta. Make a drawing of the aortic root, indicating the cusps as they appear, and count every 10 µm section that are cut from point zero onwards.
- When a second cusp appears, slightly tilt the specimen again away from the cusp to align the specimen with the third cusp. The level difference between the cusps should not exceed 50 µm. Start to collect sections on slides from level 90 µm and onwards.
- Collect sections according to the slide planning in Figure 3. The collection of sections may be started from 190 µm if the aortic root is more than 50 µm tilted, to allow further space to align the root in a straight position. Continue sectioning until reaching level 800 µm from point zero. If there are still visible plaques at this level, the collection could be expanded to 1,000 µm.
NOTE: A simplified slide organization is presented in Supplemental Figure 1, which could increase sectioning speed. The optimal slide planning should be decided depending on the project plan.
- Fix the sections after collection.
- Fix the sections collected for Oil Red O staining and Picrosirius red staining of collagen in 4% formaldehyde for 10 min. Rinse in deionized water, dry, and store in room temperature until pursuing with section 4 in this protocol. If slides should be stained with Oil Red O right away and are still wet, place them in 60% isopropanol for 1 min to speed up the drying process.
CAUTION: Isopropanol is a flammable liquid that could cause serious eye irritation and may cause drowsiness or dizziness. Store in a well-ventilated place and take precautionary measures when handling. - Fixate the sections collected for immunohistochemistry or immunofluorescence in ice cold pure acetone for 10 min. Dry in room temperature for 30 min. Store sections in -20 °C.
- Fix the sections collected for Oil Red O staining and Picrosirius red staining of collagen in 4% formaldehyde for 10 min. Rinse in deionized water, dry, and store in room temperature until pursuing with section 4 in this protocol. If slides should be stained with Oil Red O right away and are still wet, place them in 60% isopropanol for 1 min to speed up the drying process.
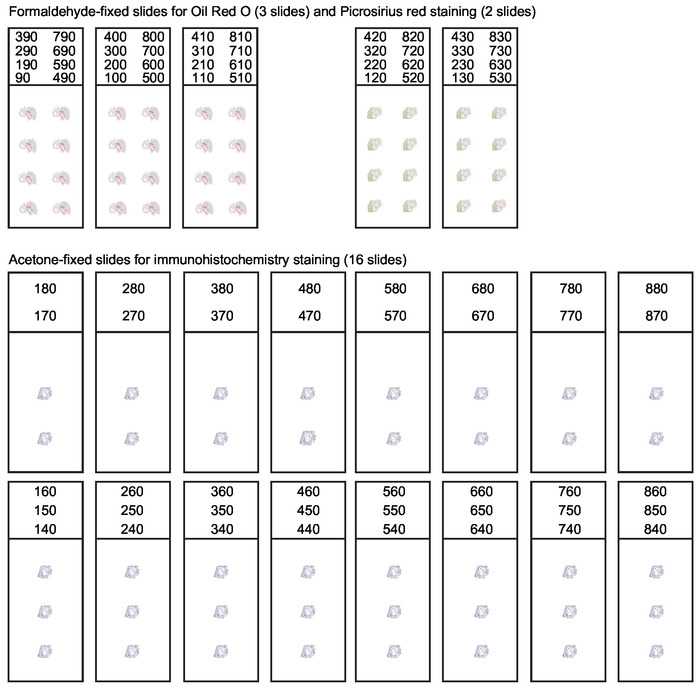
Figure 3: Organization of slides for serial sections of the aortic root. During cryosectioning of the aortic root every 10 µm thick section spanning the first 800 µm of the ascending aorta should be collected. A systematic slide organization is needed to obtain suitable sections for various applications. Analysis of lesion composition usually includes Oil Red O staining for lipids and Picrosirius red staining for collagen. Remaining sections are collected and acetone-fixed for immunohistochemistry and immunofluorescence staining. This figure has been modified from Gisterå et al30. Please click here to view a larger version of this figure.
4. Oil Red O Staining and Quantification of Atherosclerosis in Aortic Roots
- Prepare a saturated Oil Red O solution by dissolving 1 g of Oil Red O in 100 mL of isopropanol. Stir the solution in a dark bottle for 1 hour at room temperature. The saturated solution can be kept for several months.
NOTE: It is advisable to have designated laboratory equipment for Oil Red O staining since it is difficult to clean equipment that has been in contact with the solution. - Prepare a working solution by mixing 75 mL of the saturated Oil Red O solution with 50 mL of deionized water. Let stand in room temperature for 10 min. Filter through a qualitative filter paper.
- Place the slides in Oil Red O working solution for 20 min. Rinse in tap water for 5 min.
- To assist tissue visualization, stain with Mayer’s hematoxylin for 1 min. Rinse in lukewarm tap water for 5 min. All nuclei should now be stained in blue color, adjust staining time to optimize the result.
- Mount slides in an aqueous mounting medium (e.g., Kaiser’s glycerol gelatin). Warm Kaiser’s glycerol gelatin to 40 °C to make it fluid before use. It is not necessary to dry the slides since the mounting medium is water based. Be careful to avoid air bubble formation when adding the cover glass.
CAUTION: Kaiser’s glycerol gelatin contains phenol, which is suspected of causing genetic defects. Use personal protective equipment as required. - Acquire digital micrographs using a camera connected to a light microscope. Usually the full vessel wall and lesion boundaries could be clearly visualized by 50 times magnification. Save high resolution images, preferably in tagged image file format (TIFF).
- Perform analysis of lesion size using a computer-assisted image analysis software system. Oil Red O is a lysochrome diazo dye that stains neutral lipids and visualizes atherosclerotic plaques with an intense red color, which assists lesion quantification.
NOTE: The lesion quantification should be done in a blinded fashion and it is advisable that a second investigator confirms the obtained results.- Use the area quantification feature in the image analysis software to define the total vessel area by encircling the external elastic lamina of the aortic vessel wall (Figure 2B). In ImageJ, select the polygon selection tool and encircle the area by repetitive clicks. Then select measure in the analyze menu. The total vessel area is displayed in the result window.
- Continue to quantify the atherosclerotic lesions in the intimal layer of the vessel, defined by the internal elastic lamina and the luminal boundary. Usually lesions on valve cusps are excluded from the measurement27. In ImageJ, select the freehand selection tool and encircle all plaques while pressing the Alt key. Select measure in the analyze menu to display the lesion-free vessel area in the result window.
- Calculate the relative lesion area by subtracting the lesion-free area from the total vessel area and then dividing the result with the total vessel area.
NOTE: Calibrate the results in the image analysis software according to the used magnification to obtain absolute lesion area in square micrometer.
- Define the Oil Red O-stained area in the lesions by using a color threshold feature in the image analysis software to calculate the percentage of Oil Red O positive area of total lesion area.
- In ImageJ, encircle all lesion area by using the freehand selection tool while pressing the shift key. Select measure in the analyze menu to display total lesion area is in the result window.
- Select clear outside in the edit menu. Change the image type to 8-bit in the image menu.
- Set a red threshold for Oil Red O negative area by selecting threshold in the adjust submenu of the image menu. Click apply. Make the image binary by selecting this option in the binary submenu of the process menu.
NOTE: Usually Oil Red O staining varies between batches. Hence, color thresholding is only recommended within the same staining batch. The result should be presented along with a description how the threshold was determined and standardized. - Analyze the picture by selecting analyze particles in the analyze menu and click ok. Total Oil Red O negative lesion area is now displayed in the summary window. Calculate the relative Oil Red O positive area by subtracting the Oil Red O negative area from the total lesion area and then dividing with the total lesion area.
In mouse models of atherosclerosis the most prominent lesions tend to develop in the aortic root and aortic arch. This protocol describes quantification of atherosclerosis in the aortic root, the aortic arch, and the brachiocephalic artery in a single mouse. Measurable lesions in thoracic descending aorta and abdominal aorta are only present in animals with advance disease. In this protocol, these parts are not analyzed for atherosclerotic burden, but saved for subsequent analysis of mRNA levels or other analyses. Serial sections of atherosclerotic lesions in the aortic root are usually displayed in a graph with lesion size on the y-axis and distance to the aortic sinus on the x-axis28. True cross-sections are crucial for lesion size quantification. Oblique sections can overestimate lesion sizes and a tilting of only 20° could overestimate the absolute lesion surface by 15%29. However, calculating the lesion fraction of total vessel area makes the result less sensitive to possible angle differences during sectioning (Figure 4A). An appropriate statistical method to detect differences between groups is usually a regular 2-way analysis of variance (ANOVA). Bonferroni post-tests are then carried out to detect differences at certain levels. Fisher's least significant difference could also be used as a follow-up test to ANOVA. It reduces the likelihood of type II statistical errors, but do not account for multiple comparisons. In addition, it could be illustrative to calculate area under the curve or the average lesion size per mouse and present the data in a dot plot to further visualize individual variation within the groups (Figure 4B).
Oil Red O is a fat-soluble bright red diazo dye, which stains neutral lipids. Polar lipids in cell membranes are not stained. Oil Red O staining can be performed on fresh, frozen, or formalin-fixed samples, but not on paraffin-embedded samples due to the removal of lipids in the required deparaffinization process. A quantification of lesional lipid accumulation could be performed by color thresholding the Oil Red O positive area of total lesion area (Figure 4C). Hematoxylin produces a blue staining of cell nuclei, which is helpful to visualize plaque morphology. The right and left coronary arteries usually diverge from the aorta around 250 µm from the aortic sinus27, which often coincide with the most prominent lesion sizes. Cross-sections from this region is often displayed as representative results (Figure 4D).
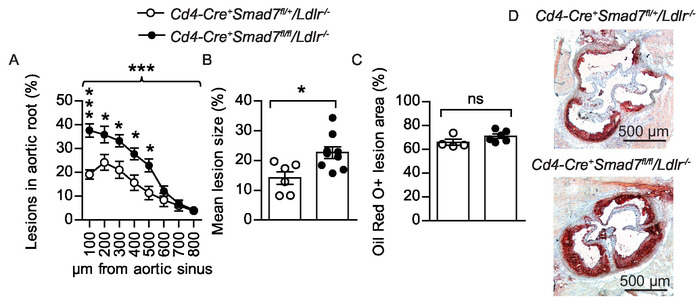
Figure 4: Atherosclerotic lesions in the aortic root. (A) Twenty-eight weeks old male bone marrow chimeras fed Western diet for eight weeks were evaluated to determine the effect of Smad7-deficient T cells on atherosclerosis development. Experimental Ldlr-/- chimeras received Cd4-Cre+Smad7fl/fl bone marrow and controls received Cd4-Cre+Smad7fl/+ bone marrow. The graph shows quantification of atherosclerotic lesion area from eight consecutive sections, 100 – 800 µm from the aortic sinus displayed as lesion fraction of total vessel surface (Cd4-Cre+Smad7fl/+/Ldlr-/- n=6, Cd4-Cre+Smad7fl/fl/Ldlr-/- n = 9, 2-way ANOVA with Bonferroni’s post test, graph shows mean ±SEM, braces indicate significance level for strain comparison). (B) The combined dot plot and bar graph shows the mean atherosclerotic lesion area from the aortic root sections (Cd4-Cre+Smad7fl/+/Ldlr-/- n=6, Cd4-Cre+Smad7fl/fl/Ldlr-/- n = 9, Student’s t-test) (C) Fraction of Oil Red O-stained area in the lesions (Cd4-Cre+Smad7fl/+/Ldlr-/- n = 4, Cd4-Cre+Smad7fl/fl/Ldlr-/- n = 6, Student’s t-test, ns=non-significant) (B–C) Dots represent individual mice and bars show mean ±SEM. (D) Representative micrographs showing Oil Red O staining (in red color) of neutral lipids in the aortic root 300 µm from aortic sinus (50x magnification), Scale bar = 500 µm. *p ≤ 0.05, ***p ≤ 0.001. This figure has been modified from Gisterå et al.31. Please click here to view a larger version of this figure.
Oil Red O could be used for staining of en face prepared aortas, but this protocol uses Sudan IV, another convenient fat-soluble diazo dye. Sudan IV clearly visualizes atherosclerotic plaques in an orange-red color by staining lipids, triglycerides, and lipoproteins. Removing the dark background in representative images of the en face aortic arches could enhance the visual display (Figure 5A). Usually lesion size is normally distributed within groups, allowing statistical testing with Student’s t-test between groups. A dot plot that shows both individual mice and the mean, which is compared between groups, is an informative way to display the results (Figure 5B-C). Since the variation within groups typically is different between locations in the vascular tree, separate power calculations are usually needed. Unnecessary variation can be avoided by method proficiency and protocol standardization. Obtaining statistically significant results is important, but the biological relevance for an observed difference always needs to be considered as well.
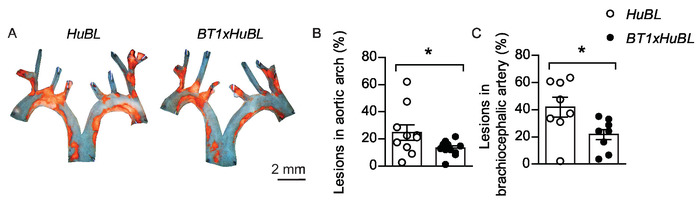
Figure 5: Atherosclerotic lesions in aortic arch and brachiocephalic artery. (A) Representative en face micrographs of aortic arches with lipid-laden plaques stained with Sudan IV (in orange color) from 20 weeks old mice fed Western diet for ten weeks, visualized together. Scale bar = 2 mm. Human APOB100-transgenic Ldlr-/- (HuBL) mice were used as controls and the experimental group consisted of TCR-transgenic mice with LDL-reactive T cells (BT1) crossbred to HuBL mice. (B) Atherosclerotic lesions in the aortic arch (HuBL n = 10, BT1xHuBL n = 12; Student’s t-test). (C) Atherosclerotic lesions in the brachiocephalic artery (HuBL n = 8, BT1xHuBL n = 9, Student’s t-test). (B–C) Dots represent individual mice, bars show mean ±SEM. *p ≤ 0.05. This figure has been modified from Gisterå et al.32. Please click here to view a larger version of this figure.
Supplemental Figure 1: Alternative organization of slides for serial sections of the aortic root. A simplified systematic slide organization for collection of sections from the aortic root. The collection enables Oil Red O staining for lipids and immunohistochemistry or immunofluorescence staining. Dedicated slides for Picrosirius red staining of collagen are omitted. Please click here to download this file.
