The full result of this study is available in the original paper published23. Parkinson’s disease subjects (n = 67) were recruited and completed the assessment. However, 5 cases failed to complete the visual search task as they wore progressive lens incompatible with the eye tracker and their data was discarded. The mean age of the subjects was 58.9 years (SD = 7.5 years) with a male to female ratio of 1.7:1. 62 healthy age-, sex-, and education-matched controls were recruited for comparison.
Cognitive and eye movement parameters
Consistent with other previous studies24, the Parkinson’s disease group showed poorer performance in multiple cognitive tasks as compared to the control group (Table 1). Using the in-house algorithm for classification of the visual search task data, fixations and saccades are identified and extracted for calculation and analysis. It was found that the disease group had a smaller mean saccadic amplitude (16.36° ± 2.36) as compared to controls (17.27° ± 2.49; p = 0.037). The mean fixation duration was not significantly different between the groups (216.58 ms ± 31.64 vs, 211.59 ms ± 24.90; p = 0.331) (Table 2).
Correlation between eye movement parameters and cognitive function
After adjusting for covariates, there were negative correlations found between the mean fixation duration and the performance in verbal recognition memory score (Recognition and Discrimination scores; F = 5.843, t = -2.417, p = 0.017 and F = 12.771, t = -3.574, p = 0.001, respectively), pattern recognition memory (F = 5.505, t = -2.346, p = 0.021) and categorical verbal fluency test in the categories of fruit (F = 5.647, t = -2.376, p = 0.009) and vegetable (F = 9.744, t = -3.122, p = 0.002). (Table 3). However, there was no significant interaction found in these correlations between the disease and control group, suggesting that the correlations are not specific to the disease group. It is speculated that as the control of visual fixation and the correlated cognitive functions commonly involve temporal and parietal regions of the brain with a predominantly cholinergic basis, pathological changes to these neuroanatomical and biochemical mechanisms may explain the findings.
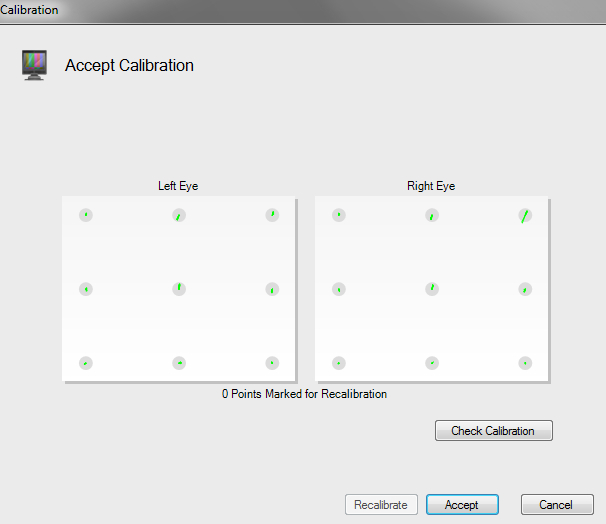
Figure 1: A calibration plot of the eye tracker. The plot shows the result of the calibration. The length of each green line indicates the difference between the gaze point calculated by the eye tracker and the actual dot position. As all the green lines fall within the grey circles and there is no missing point, the quality of this calibration is acceptable. Please click here to view a larger version of this figure.
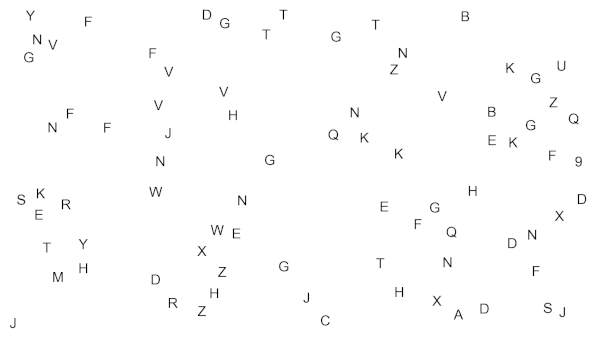
Figure 2: An example of a trial of the visual search task. Display of a non-linear array of 80 stimulus items, of which there is 1 number among 79 distracter alphabets. Please click here to view a larger version of this figure.
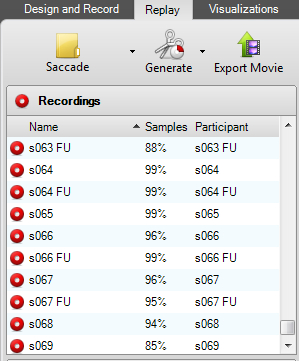
Figure 3: The interface to check the overall sampling percentage. In the Replay section of the computer program, the Samples Percentage, which denotes the percentage of time that the eyes are successfully located by the eye tracker during the visual search task, could be checked for each subject. Please click here to view a larger version of this figure.
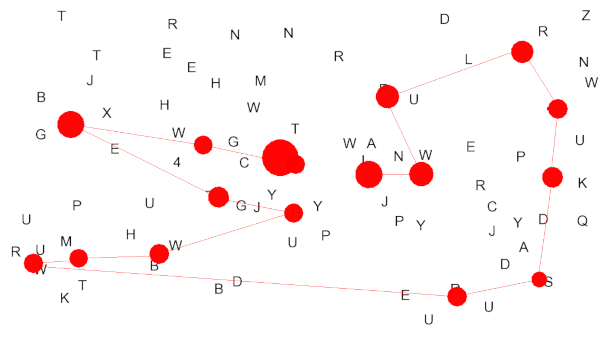
Figure 4: An example of a visualized scan path from the visual search task. The scan path during this trial was visualized, with the red straight lines representing the saccadic eye movement and the red dots for visual fixations. Note that the end of each visual fixation is followed by a saccade and vice versa in a normal scan path. Please click here to view a larger version of this figure.
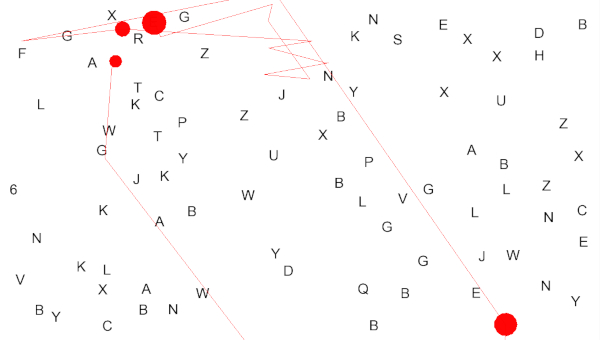
Figure 5: An example of a grossly erroneous visualized scan path. This example of a grossly erroneous scan path is taken from a subject wearing a pair of incompatible progressive lens. In contrast to the normal scan path in Figure 4, the red lines (saccade) run in zigzag and fall out of the computer screen. The fixation points are not on either the alphabets or the number. Please click here to view a larger version of this figure.

Figure 6: The data export interface in the computer program. This shows the interface where the subject and the kind of the eye tracking data captured can be selected for data export. In our experimental paradigm, the x and y coordinate, in pixels, of the eyes position on the screen at every time point will be used for data analysis. Please click here to view a larger version of this figure.
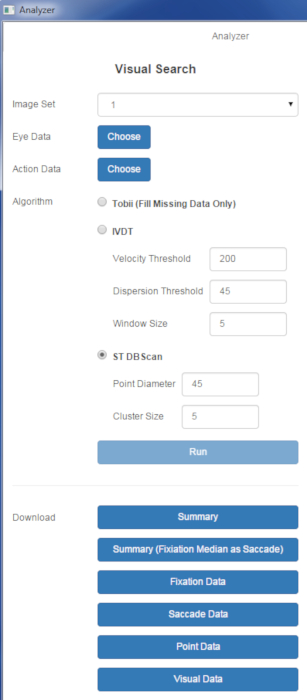
Figure 7: The interface of the Visual Search Analyzer. This shows the interface of the in-house analysis program for eye tracking data. Please click here to view a larger version of this figure.
| Control group | Parkinson's group | p-value | |
| Global Cognitive scales | |||
| MMSE | 28.53 (1.63) | 28 (1.84) | 0.09 |
| MoCA | 27.10 (2.25) | 26 (2.34) | 0.009* |
| Specific Cognitive tests – Frontal executive & Frontal-temporal | |||
| Stocking of Cambridgea | 1.16 (0.14) | 1.24 (0.19) | 0.018* |
| Stroop testb | 1.24 (1.77) | 1.36 (1.65) | 0.697 |
| Verbal fluency – animalb | 0.92 (1.47) | 0.26 (1.31) | 0.01* |
| Verbal fluency – fruitb | -0.71 (0.74) | -1.01 (0.79) | 0.028* |
| Verbal fluency – vegetableb | -0.66 (1.04) | -1.11 (0.90) | 0.011* |
| Specific Cognitive tests – Verbal Memory (Hong Kong List Learning Test) | |||
| Total learningb | 0.03 (0.90) | -0.30 (0.87) | 0.037* |
| 10 minutes delay free recallb | -0.17 (0.90) | -0.44 (1.10) | 0.131 |
| 30 minutes delay free recallb | -0.19 (0.90) | -0.39 (1.04) | 0.206 |
| Recognition scoreb | 0.10 (1.00) | 0.15 (0.73) | 0.722 |
| Discrimination scoreb | -0.05 (1.02) | -0.13 (0.97) | 0.636 |
| Specific Cognitive tests – Visual spatial memory | |||
| Pattern recognition memoryc | 91.33 (9.40) | 87.77 (10.20) | 0.045* |
| Specific Cognitive tests – Attention/Working memory | |||
| Spatial spand | 6.15 (1.10) | 5.65 (1.17) | 0.016* |
Table 1: Comparison of cognitive scores between two groups using independent sample t-test. MMSE, Mini-Mental State Examination; MoCA, Montreal Cognitive Assessment; *– p<0.05 a – mean choices to correct; b – scores transformed into z-score; c – percentage correct; d – span length. This table has been reproduced from23.
| Control group | Parkinson's disease group | p-value | |
| Mean fixation duration, in miliseconds (SD) [Range] | 211.59 (24.90) [165.77 – 264.63] | 216.58 (31.64) [145.43-312.68] | 0.331 |
| Mean saccadic amplitude, in degrees (SD) [Range] | 17.27 (2.49) [13.34 – 22.99] | 16.36 (2.36) [11.66-23.20] | 0.037* |
Table 2: Comparison of eye tracking parameters between two groups using independent sample t-test. * – p < 0.05. This table has been modified from23.
| Source | Dependent Variable | df | F | B | Beta | Std. Error | t | p-value |
| Mean fixation duration | Verbal fluency – fuit | 1 | 5.647 | -0.006 | -0.227 | 0.002 | -2.376 | 0.009* |
| Verbal fluency – vegetable | 1 | 9.744 | -0.009 | -0.288 | 0.003 | -3.122 | 0.002* | |
| Recognition score | 1 | 5.843 | -0.007 | -0.215 | 0.003 | -2.417 | 0.017* | |
| Discrimination score | 1 | 12.771 | -0.011 | -0.314 | 0.003 | -3.574 | 0.001* | |
| Pattern recognition memory | 1 | 5.505 | -0.071 | -0.215 | 0.03 | -2.346 | 0.021* |
Table 3: Correlations between cognitive scores and eye-tracking parameters using General Linear Model: Significant findings only. * – p < 0.05. This table has been reproduced from23.

Supplemental File 1: Codes related to the trial image design. Please click here to download this file.

Supplemental File 2: Codes related to the actual run of the visual search task. Please click here to download this file.

Supplemental File 3: Codes related to the software (e.g., analyzer program). Please click here to download this file.

Supplemental File 4: Codes related to the ST-DBSCAN algorithm used for classifying eye movement metrics. Please click here to download this file.
