Eight to ten-week-old mice were anesthetized with isoflurane and intubated. After the animal was under anesthesia, the left thoracic region was shaved and sterilized with ethanol, and the heart was exposed for LAD ligation. The left coronary artery was occluded by firmly knotting the suture under the artery (diagram representation Figure 1A). After a successful infarction (indicated by the paling of the left ventricular free wall), a direct injection of 100 µg of Luc or Cre modRNA dissolved in sucrose citrate buffer was delivered directly into the myocardium at three different sites (Figure 1B) surrounding the injury area using an insulin syringe. The MI procedure with modRNA injections lasted for 30−45 min per animal. The animals showed approximately 90% survival rate postprocedure. After the procedure, the chest and the skin were firmly sutured in layers and the animal was removed from ventilation as soon as it started breathing normally.
After conducting the LAD ligation and subsequent delivery of Luc modRNA injection, we validated the Luc modRNA transfection by checking for Luc protein expression 24 h postinjection using a bioluminescence imaging system (Figure 2A). We established in previous publications that although the protein expression can be seen until day 6 posttransfection, the highest transfection efficiency of modRNA is observed at 24 h8. Similarly, we successfully detected the Luc signal in the heart treated with Luc modRNA injection (1.76 x 108) compared to the mice injected with sucrose citrate buffer after MI (3.0 x 105) (Figure 2B).
Further, we sought to validate the modRNA expression by checking its translation and biodistribution in a transgenic Rosa26mTmG mouse. This mouse model system expresses the cell membrane-localized tdTomato (mT) fluorescence expression in all body cells/tissues and changes to cell membrane-localized EGFP (mG) fluorescence expression upon Cre recombination. Thus, to observe the expression of the Cre modRNA, 100 μg Cre modRNA was injected directly into the myocardium post-MI in Rosa26mTmG male and female mice, and the animals were sacrificed 24 h postsurgery. Hearts were fixed and processed for immunostaining with cardiomyocyte marker cTNI and nuclear marker DAPI (Figure 3A). Successful Cre expression was evident due to the appearance of green colored cells (Figure 3B), which were a result of recombination with the Cre modRNA delivered to the mouse, represented by the change of the tdTomato color to EGFP around the Cre injection site (Figure 3C).
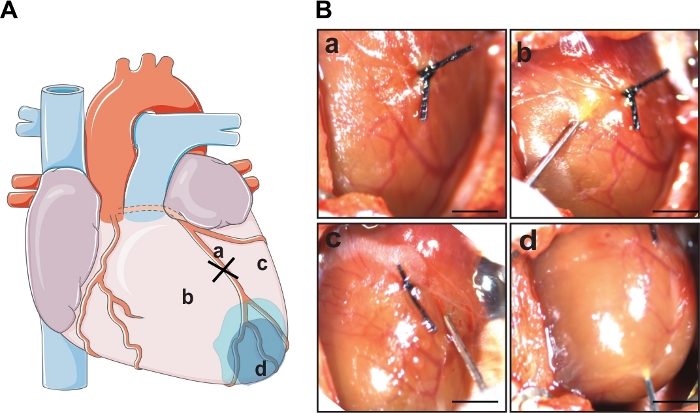
Figure 1: LAD ligation and cardiac delivery of modRNA. (A) Schematic diagram showing the area of LAD ligation and three sites of modRNA injection. (B) Representative images of the whole mouse heart post a successful MI induced by permanent ligation (a) and sites of modRNA injection following the MI. The 100 µg of modRNA dissolved in 60 µL of sucrose citrate buffer was delivered in the border zone area surrounding the infarction, two on either side of the ligation (b,c) and one in the apex (d). Scale bar = 1 cm. Please click here to view a larger version of this figure.
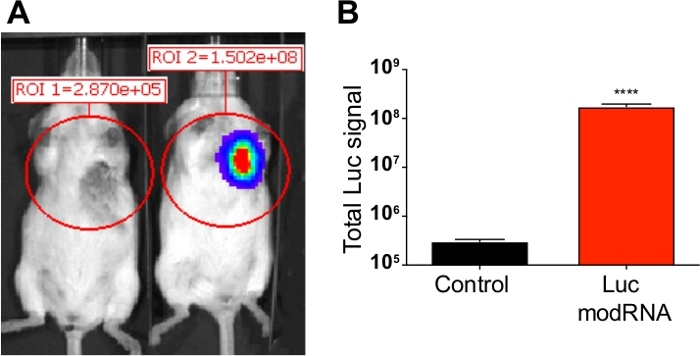
Figure 2: Luc expression analysis post modRNA injection. Sucrose citrate buffer containing 100 µg of Luc modRNA was injected directly into myocardium of CFW mice in an open-chest surgery. The bioluminescence imaging system was used to calculate Luc protein expression at 24 hours after injection. (A) Comparative bioluminescent images of control mice (transfected with buffer only) vs. mice injected with Luc modRNA. (B) Quantification of Luc signal compared with the control mice measured after 24 hours using bioluminescence imager. Error bar represents SEM with p < 0.0001. Please click here to view a larger version of this figure.
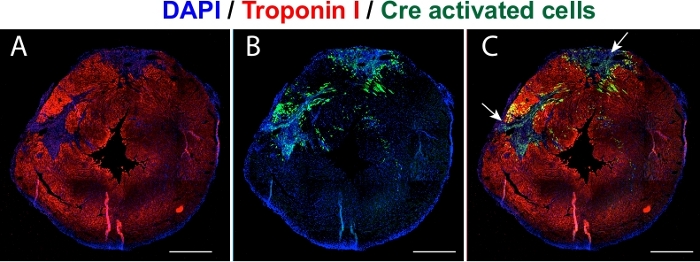
Figure 3: Validation of Cre expression in vivo. Representative images of transfected heart cross sections (short-axis view) validating the expression of Cre modRNA in Rosa26mTmG mouse 24 hours postinjection. (A) The cardiomyocytes immunostained with cTNI (red). (B) Green colored cells represent the Cre transfected cells. (C) Merged image showing Cre activated cells around the two injections. Blue is the nuclear stain DAPI. Scale bar = 1 cm. Please click here to view a larger version of this figure.
