This study was approved by the University of Southern California Institutional Review Board and adhered to the tenets of the Declaration of Helsinki.
1. Setup of Gas Non-rebreathing Apparatus
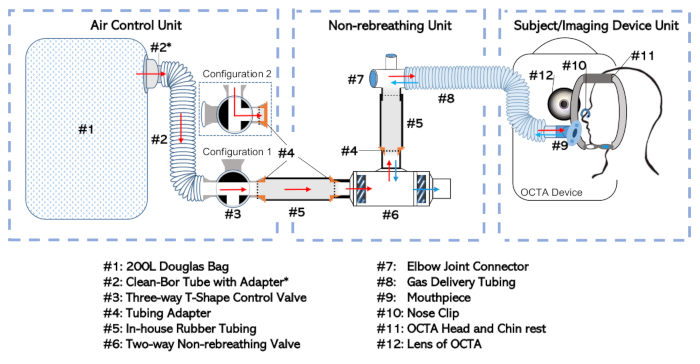
Figure 1: Diagram of the non-rebreathing apparatus. The full setup has been broken into three separate units according to their function and the frequency with which they are dealt with independently. These include: the Air-Control Unit, the Non-rebreathing Unit, and the Subject/Imaging Device Unit Please click here to view a larger version of this figure.
- Apparatus assembly
- Connect the Douglas bag (Figure 1, #1) to the three-way valve (#3) at a selective inlet port via the 35 mm inner-diameter tube (#2; see Table of Materials) with adapter (#2*). This combination will be called the “Air Control Unit” as shown in Figure 1.
- Connect the two-way non-rebreathing valve (#6) to the elbow joint connector (#7) at the non-rebreathing valve’s mouth port. Form the connection using a rubber tube (#5) fitted with an adapter (#4).
- Connect the elbow joint to the gas delivery tubing (#8). This setup, including the non-rebreathing valve (#6), in-house tubing (#5), adapters (#4), elbow joint (#7), and gas delivery tubing (#8) will be called the “Non-rebreathing Unit”.
NOTE: Minimize the amount of dead space between the subject’s mouth and the diaphragm of the two-way non-rebreathing valve (#6). - Connect the Air Control Unit at the outlet port of the three-way valve (#3) to the Non-rebreathing Unit at the inlet port of the two-way non-rebreathing valve (#6). Make the connection using additional rubber tubing (#5) and adapters (#4) as those described earlier that allow the pieces to be inserted into one another.
- Seal all loose connections by wrapping the joints with sealing tape to ensure a hermetic fit.
- Connect the gas delivery tubing (#8) at its open end to a mouthpiece (#9) as shown in the Subject/Imaging Device Unit of Figure 1.
NOTE: This step (1.1.6) can be deferred until the subject testing is ready to begin (Step 3.5).
- Preparation of the Air Control Unit for gas non-rebreathing
- Isolate the Air Control Unit by disconnecting it from any in-house tubing (#5) or adapters (#4) if it is not already separated.
- Ensure the Douglas bag (#1) is empty or empty the Douglas bag (#1) of any air by systematically rolling-up the bag from the distal end towards the bag’s inlet port with the three-way valve (#3) set to Configuration 1 as shown in Figure 1.
- Fill the Douglas bag (#1) with the appropriate gas mixture.
- If only room-air non-rebreathing is intended, set the three-way valve to Configuration 2 (shown in Figure 1) and do not fill the Douglas bag (#1). Otherwise continue with the steps that comprise Step 1.2.3.
- Connect the Air Control Unit (shown in Figure 1) at the outlet port of the three-way valve (#3) to a gas-cylinder (containing the desired air-mixture) using the appropriate adapters and tubing. Use a cuff adapter to mount a 1/8” gas filling tube to the outer diameter of the three-way valve (#3).
- Set the three-way valve assembly to Configuration 1 (as shown in Figure 1) to allow the intended gas to flow from the storage cylinder into the Douglas bag (#1). Open the gas cylinder.
- Once the Douglas bag (#1) is filled to the intended volume (usually half-filled), close the gas cylinder outlet and set the three-way valve to Configuration 2, which isolates the gas within the Douglas bag (#1). Disconnect the Air Control Unit from any tubing used to fill the Douglas bag (#1).
2. Preparing the Subject for Imaging
- After the subject consents to participate in the study, sit the subject behind the OCTA imaging device. Explain the testing procedures to the subject.
- Confirm the subject’s medical history to ensure that the subject has no existing medical conditions that increase the risk of participating in the study.
NOTE: Pre-existing cardiovascular or pulmonary diseases are risk factors for which subjects may be excluded from participating. It is essential that the subject understand that they can stop the procedure at any time for any reason such as feeling lightheaded or some additional unexpected discomfort. - Determine the eye to be assessed as per the testing protocol. One eye only may be imaged to limit the testing time and minimize the potential discomforts from the gas non-rebreathing.
- Consider eye dilation if the subject has a pupil size of about 2.5 mm or less. Although dilation is not mandatory, it enhances the chances of acquiring good quality images. To dilate, instill one drop each of 0.5% proparacaine hydrochloride ophthalmic solution, 1% tropicamide ophthalmic solution and 2.5% phenylephrine hydrochloride ophthalmic solution. Full dilation should occur within 10–15 min.
3. Gas Provocation Experiment and Image Acquisition
- Create a profile for the patient in the OCTA machine.
- Wear gloves.
- Wipe down the OCTA head and chin rest with an alcohol swab to disinfect the setup.
- Free the mouthpiece (#9) from its sterile packaging.
NOTE: Refrain from touching the mouthpiece as much as possible as this component makes direct contact with the mucus lining of the mouth of the subject - Connect the mouthpiece (#9) to gas delivery tubing (#8)
- Place a pulse oximeter on the subjects’ finger and begin monitoring oxygen saturation levels and pulse.
NOTE: Once the subject begins breathing the desired air mixture, the pulse oximeter should be continuously monitored by the examiner. If the oxygen saturation of the subject drops below 94%, the experiment should be stopped, as a safety precaution, and the subject observed until they return to baseline. - Adjust the height of the OCTA setup so that the subject can easily rest their chin on the chinrest (#11) without overextending or flexing their neck.
- Loop the gas delivery tubing (#8) with mouthpiece (#9) attachment through the head and chin rest with the mouthpiece (#9) facing the patient. Have the tubing loop through the machine oppposite the side of the eye that the subject is having imaged.
- Insert the mouthpiece into the patient’s mouth. Encourage the subject to practice breathing through the non-rebreathing setup to create familiarity with the apparatus. Ensure the subject takes deep breathes to facilitate gas exchange.
- Place the nose clip (#10) on the subject to ensure they are breathing through the mouthpiece.
- Keep the three-way valve on Configuration 2 or change it to Configuration 1 depending on whether images are being acquired for exposure to room air or a specific gas mixture, respectively. For future reference, note the time as the start of gas inhalation.
- Have the subject place their chin on the right or left section of the chinrest (#11) according to the eye selected for imaging.
- Ensure they move their head forward until their forehead is in firm contact with the headrest (#11).
- Capture the OCTA scan of interest as determined by the testing protocol. In this study, three 3 mm x 3 mm images centered on the fovea were captured after 1 min of gas breathing.
- Have the subject keep their head facing forward and still while fixating on the target in the center of their view
- In the live image seen in the iris view, center the scan.
- Bring the iris into focus by moving the chinrest in or out using the left-right arrows.
- Make sure the foveal dip is centered in the OCT scan, which should occur by default.
- Take an image. Scanning will usually last several seconds on an OCTA machine.
- View the OCTA image after the completion of the scan and ensure it is of adequate quality. Signal strength should be a 7 or better on a 10-point scale provided by the OCTA manufacturer.
- Select save or rescan the eye.
- Repeat steps 3.14.1–3.14.7 for as many scans are desired.
- Allow the subject to sit back from the machine. Remove the nose clip (#10) and the mouthpiece (#9) when no more scans of the eye with this gas mixture are needed.
- Allow subjects a 2 min break before starting CO2 gas provocation experiments.
- Fill the Douglas bag with the first desired air mixture (consisting of 5% CO2, 21% oxygen and 74% nitrogen) as specified in step 1.2. The three-way valve will be in Configuration 2 after this step.
- Complete gas non-rebreathing apparatus setup by connecting the Air Control Unit to the Non-rebreathing Unit as shown in Figure 1 and described in step 1.1.4. Make sure all joints are airtight with sealing tape.
- Repeat steps 3.9–3.14, but now set the three-way valve to Configuration 1 when directed in step 3.11.
- Give subjects a 10 min break after the CO2 gas provocation to allow a return to baseline.
- While the subject is on break, fill the Douglas bag with 100% O2 according to step 1.2.
- Repeat steps 3.17–3.18 to perform the experiment under 100% O2 gas provocation conditions.
4. Experimental Clean Up
- Discard the disposable elements of the setup: the subject’s mouthpiece (#9) and nose clip (#10).
- Clean the head and chin rest (#11) using an alcohol swab. Wipe the subject chair, OCTA table and OCTA handles with a disinfectant wipe to remove any errant saliva.
- Disconnect the setup into its base components—the Air Control Unit and Non-rebreathing Unit—at the three-way valve (#3).
- As no air exhaled from the subject should have reached the elements of the Air Control Unit, empty the Douglas bag according to step 1.2.2 and place in a location for future retrieval. Disconnect the clean-bor tube (#2) with adapter (#2*) and three-way valve (#3) from the Douglas bag if desired for easier storage. This completes the Air Control Unit clean up.
- Remove the gas delivery tubing (#8) from the Non-rebreathing Unit by disconnecting it from the elbow joint (#7). Disconnect the in-house rubber tubing (#5) and tubing adapters (#4), from the two-way non-rebreathing valve (#6). Then do the same from the elbow joint (#7) by removing the sealing tape and detaching the parts by pulling them apart.
NOTE: More extensive cleaning of the two-way non-rebreathing valve may be facilitated by disassembling it to remove the internal diaphragms for additional care. - Prepare a disinfectant bath for cleanup of the reusable components
- Fill a container large enough to submerge the gas delivery tubing (#8) with an appropriately diluted and well mixed detergent disinfectant. In this case, dilute the detergent with water to a ratio of 1:6425.
- Soak the gas delivery tubing (#8), two-way non-rebreathing valve (#6), elbow joint (#7), in-house rubber tubing (#5) and tubing adapters (#4) in the prepared disinfectant bath for at least 10 min.
- Remove all parts after the bath is over and rinse them thoroughly with water.
- Place them on a paper towel on a clean countertop to be air-dried.
- Once air drying has completed, dispose of the paper towel and place all components away for storage.
5. OCTA Data Export and Analysis
- OCTA data export
- Export OCTA data by inserting a removable media device of choice into the OCTA computer. Find the subject and scan of interest.
- Select Export to create a zip folder containing the subject of interest’s data in a .bmp format on the removable media device.
- OCTA data analysis
- Organize the OCTA data on a laboratory computer with the ability to perform additional image analysis and processing.
- Use a custom script to suppress noise with a global thresholding technique and perform additional feature extraction. Binarize and skeletonize the OCTA images.
- On the post-processed images, calculate the vessel skeleton density (VSD)19,26, a dimensionless measure of the total linear length of vessels in an image calculated by the following equation performed on a binarized skeletonized image of the OCTA:
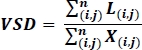
where i and j refer to pixel coordinate (i,j), L(i,j) refers to white pixels representing decorrelation, X(i,j) refers to all pixels, and n refers to the dimensions of the pixel array, which can be assumed to be n x n pixels19,26. The denominator of this equation represents the total number of pixels which is calculated as written from the skeletonized image, but can be thought of as representing the physical area of the entire image.
The output from this experiment consists of the manual readings taken from the pulse oximeter, the timing noted for gas exposure or OCTA scanning and the raw OCTA imaging data. An OCTA image consists of the OCT B-scans and the decorrelation signal associated with each B-scan. The data parameters are given by the specifications of the device. A swept source laser platform OCTA machine with a central wavelength of 1040–1060 nm was used. The images provide a transverse resolution of 20 µm and optical axial resolution of 6.3 µm. Most often, the OCTA data is presented in a 2D enface format as has been shown in the representative Figure 2. Many metrics exist for quantifying this data in a way that allows for comparisons between subjects and among different conditions. A representative metric, vessel skeleton density (VSD), is shown together with full retinal angiograms in Figure 2. As the capillaries vasoconstrict and vasodilate in response to the gas exposure, the capillary density also changes. Hypercapnic conditions are expected to result in an increase in VSD and hyperoxic conditions are expected to result in a decrease in VSD when compared to room air conditions.
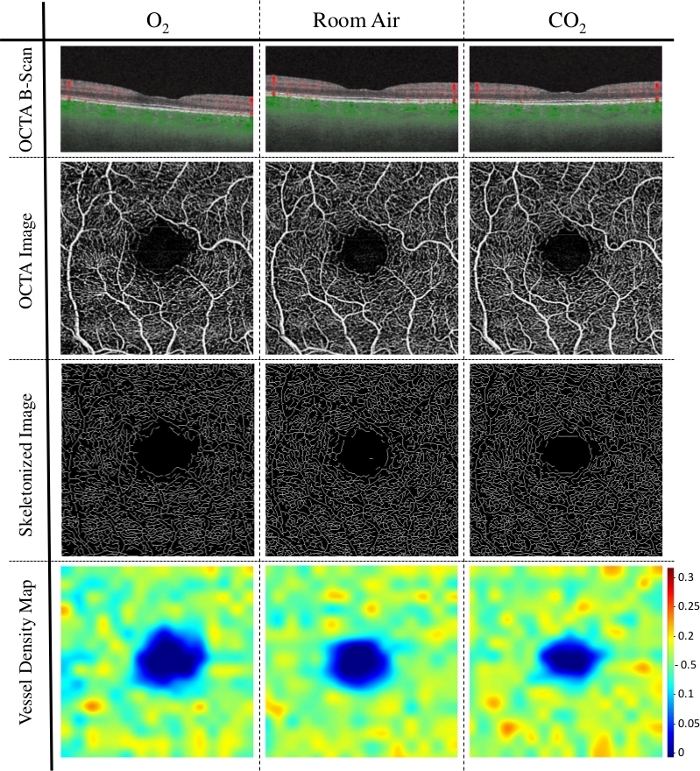
Figure 2: Representative results of vessel skeletal density (VSD) in hyperoxic, room air, and hypercapnic conditions. This graphic shows the 3 mm x 3 mm OCTA angiograms and vessel density findings of a healthy 76 year-old female subject. Row 1 shows a single representative horizontal OCT B-scan through the fovea with decorrelation signal above the retinal pigment epithelium represented by red for each of the gas breathing provocation conditions—100% O2, room air and 5% CO2 respectively. Row 2 consists of a single OCTA enface image constructed from 256 OCTA B-scans, one of which is shown in row 1. Row 3 consists of those same OCTA images in Row 2 after post-processing in which the vessels were binarized and skeletonized. Row 4 consists of a heat map showing VSD calculated locally from the images in row 3. Note that the total VSD and relative number of local VSD hot spots increases as one progresses in the columns from left to right. Please click here to view a larger version of this figure.
