Here, we consider two example cases after completion of the protocol: one with full recovery of the baseline level of ADL function at discharge, and one with no or partial recovery.
Discharged with baseline level of ADL function
In this group of patients, two ADL function trajectories were possible, as shown in Figure 1: patients who maintained their ADL score throughout hospitalization (Trajectory A) and those whose score at hospitalization was lower than at baseline, but who regained their baseline level of function by discharge (Trajectory B). Patients of either trajectory discharged with their baseline ADL function (had an 83.8% and 67% chance of maintaining it 1 month and 1 year after discharge, respectively. In this study, the 1-year mortality rate was 17.8% in this group of patients and there was no difference therein between patients who followed trajectory A and those who followed trajectory B11.
Discharged with new or additional disability in ADL
In our cohort, three types of cases were identified, as shown in Figure 2: patients who retained their baseline independence on admission to the hospital but showed deterioration during hospitalization and did not regain full independence thereafter (trajectory C); patients who lost their baseline independence prior to hospitalization for the acute problem and did not regain it during hospitalization (trajectory D); and patients who showed deterioration of independence both prior to and during hospitalization, and did not regain full independence (trajectory E)19. Of the patients discharged with new or additional disabilities in ADL, 33.5% recovered their baseline level of ADL function within the first month after discharge, and 30.1% did so within the first year. The 1-year mortality rate was 41.3% for these patients. There was no significant difference between patients who followed trajectory C and those who followed trajectory D11.
Possible errors during execution of the protocol
Our protocol is simple to implement. Errors are most likely to occur when determining the baseline ADL score, especially when it is obtained through interviews with patients. Some patients may underestimate or overestimate their prior level of functional independence at home. Furthermore, patient recall may be distorted by cognitive impairment. Considering the high prevalence of cognitive impairment among those in geriatric acute care wards, we recommend questioning the family, nurses working in the home or nursing home, or the attending physician to obtain the most accurate baseline ADL score. This questioning is mostly done by telephone after hospital admission.
Examples of results obtained at Bordeaux University Hospital
The present protocol was implemented in 2017 and applied to all patients over 75 years of age. During the year since the implementation of the protocol, loss of functional independence was observed less often. In 2016, of the 699 hospitalized older patients to whom the protocol was applied, 25.97% showed a loss of functional independence, compared to 19.48% of 852 patients in 2019.
Although systematic application of the protocol to all hospitalized geriatric patients was required, data were not consistently entered in the medical records. In 2017, only 36.78% of medical records mentioned ADL data; in 2019, these data were present in 51.26% of medical records. Thus, health professionals in the hospital should be encouraged both to carry out the protocol and record the patient outcomes.
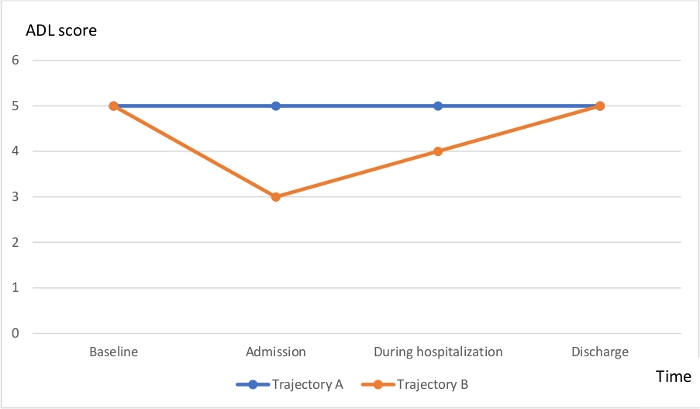
Figure 1: Favorable trajectories of ADL dependence during an acute medical problem, from baseline to post-event status. Trajectory A: Mild baseline ADL dependence with no decline at any point during the event; Trajectory B: Mild baseline ADL dependence, decline during the acute event, and recovery before discharge. Please click here to view a larger version of this figure.

Figure 2: Unfavorable trajectories of ADL dependence during an acute medical problem, from baseline to post-event status. Trajectory C: Mild baseline dependence, no decline noted on admission but decline during hospital stay. Trajectory D: Mild baseline dependence, decline noted on admission, no recovery during hospital stay or at discharge. Trajectory E: Moderate baseline dependence, decline noted on admission, further decline during hospital stay, no recovery before discharge. Please click here to view a larger version of this figure.
