When a dry powder insufflator is used to deliver powder aerosol to the lung of an animal, the volume of air used is critical as it affects the safety as well as the powder dispersion efficiency. To optimize the method, different volumes of air (0.3 mL, 0.6 mL and 1.0 mL) were used to disperse the dry powder (1 mg of spray dried mannitol) and the weight of mice was monitored for 48 hours after administration (Figure 6). The use of 0.3 mL and 0.6 mL of air did not cause weight loss of the mice up to 48 h post-administration. Dispersing the powder with 1 mL of air resulted in over 5% of weight loss within 24 h, which was not fully recovered after 48 h. In this protocol, BALB/c mice of 7-9 weeks old were used. Depending on the species, the strain and age of animal, the powder properties (e.g., particle size distribution, cohesiveness and density) and the mass of powder to be administered, the volume of air to be used for efficient powder dispersion and animal tolerance may require optimization by investigators for different animal models.
Dry powder formulation prepared by spray freeze drying (SFD) was delivered to the mice using the method described above. The SFD formulation contained 0.5% of mRNA expressing luciferase protein, 5% of synthetic peptide as delivery vector and 94.5% of mannitol16. BALB/c mice were intratracheally administered with 1 mg of SFD powder containing 5 µg of mRNA and the luciferase expression in the lungs was evaluated at 24 h post-administration using in vivo imaging system (IVIS) (Figure 7). The SFD powder were dispersed in the deep lung and luciferase expression was observed. As a comparison, the SFD powder were reconstituted in PBS (to a final volume of 75 µL) and administered to mice as liquid with the same intubation procedure but a microsprayer was used instead to generate liquid aerosol16. The luciferase expression of the reconstituted formulation was significantly higher than the dry powder formulation, which could be due to the powder dissolution issue or different pharmacokinetic profile between powder and liquid form. The histological characteristics of the lungs treated with mRNA dry powder aerosol were compared with untreated control and lipopolysaccharide (LPS) treated groups (Figure 8). The lungs without any treatment illustrated a healthy presentation while the lung treated with 10 µg of LPS intratracheally showed irregular distribution of air space and inflammatory cell infiltration into the interstitial and alveolar spaces. The lungs treated with SFD powder did not show any signs of inflammation.
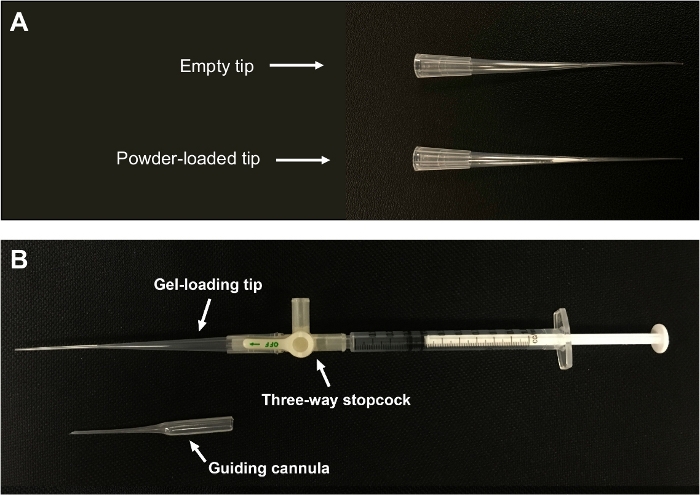
Figure 1: Custom-made dry powder insufflator.
(A) Powder is packed near the narrow end of the tip. (B) A gel-loading pipette tip is connected to a 1 mL syringe via a three-way stopcock. The figure is adapted from Liao et al.21. Please click here to view a larger version of this figure.

Figure 2: Custom-made light source for intubation.
A flexible optical fiber is connected to a LED torch by creating a small hole on the lens. Please click here to view a larger version of this figure.
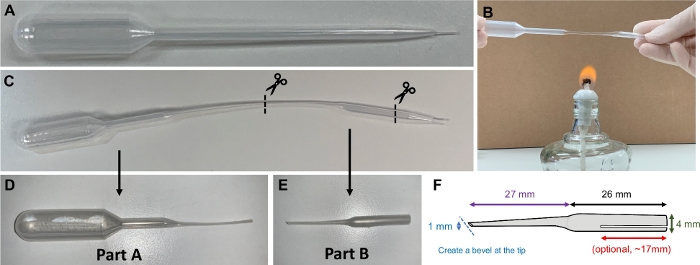
Figure 3: Guiding cannula.
(A) A 1 mL plastic Pasteur pipette is used to make a guiding cannula. (B) The pipette is softened by heating. (C) The heated pipette is stretched and cut. (D) Part A of the pipette is used as fine-tip pipette. (E&F) Part B of the pipette is used as a guiding cannula. A bevel is created to facilitate intubation procedure. A small opening (optional) can be made to increase the flexibility of the cannula. Please click here to view a larger version of this figure.
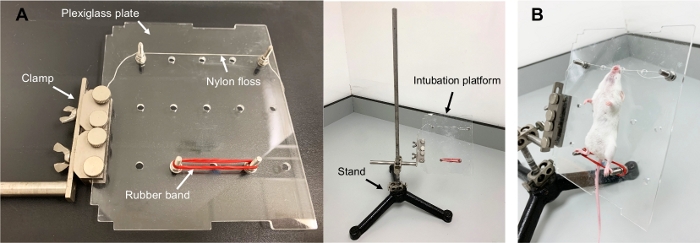
Figure 4: Intubation platform.
(A) The platform for intubation consists of a Plexiglass plate which is mounted to a stand. (B) An anaesthetized mouse is placed on the platform in a supine position, suspended by hooking its incisors with a nylon floss. Please click here to view a larger version of this figure.
Figure 5: Schematic diagram illustrating the intubation procedure.
(A) The bevel of the guiding cannula is aligned with the midline of the tracheal opening. (B) The guiding cannula is inserted into the trachea and ready for powder administration. (C) The powder-loaded tip (connected to the syringe through a three-way stopcock) is inserted into the guiding cannula which has already been placed in the trachea of the mouse. Please click here to view a larger version of this figure.
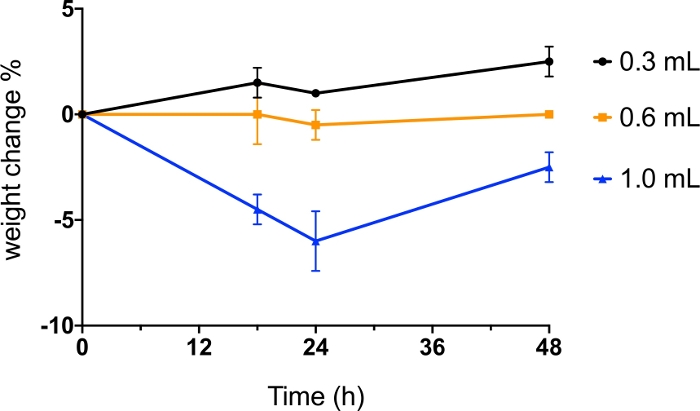
Figure 6: Intratracheal administration of dry powder with different volume of air.
BALB/c mice were administered intratracheally with spray dried (SD) mannitol powder dispersed by 0.3 mL, 0.6 mL and 1.0 mL of air. Body weight of the mice was monitored before administration and at 18 h, 24 h and 48 h post-administration. The data was presented as mean value of percentage of weight change (n=2). Please click here to view a larger version of this figure.
Figure 7: Intratracheal administration of mRNA formulation as dry powder and reconstituted liquid aerosol.
BALB/c mice were administered intratracheally with spray freeze dried (SFD) 0.5% mRNA (luciferase) formulation as powder aerosol (1 mg) using custom-made dry powder insufflator or reconstituted liquid aerosol (1 mg in 75 μL PBS) using microsprayer. Each mouse received a dose of 5 μg of mRNA. PBS (75 µL) was used as control. At 24 h post-administration (A) the lungs were isolated for bioluminescence imaging; (B) luciferase protein expression of the lung tissues were measured. The data was expressed as the mean value of relative light unit (RLU) per mg of protein, analyzed by one-way ANOVA followed by Tukey’s post-hoc test, ***p < 0.001 (n=4). The figure is adapted from Qiu et al.16. Please click here to view a larger version of this figure.
Figure 8: Histology of the lungs of mice following intratracheal administration of mRNA dry powder formulation.
(A) untreated control; mice were intratracheally administered with (B) LPS (10 mg in 25 μL PBS), and (C) spray freeze dried mRNA powder (1 mg). Slides were viewed using an upright microscope at 20x magnification (scale bar = 100 mm). The figure is adapted from Qiu et al.16. Please click here to view a larger version of this figure.
