SD-OCT is considered successful if high quality images are obtained such that ocular dimensions can be reliably measured. Here, a variety of uses of SD-OCT are illustrated using models of retinal degeneration, glaucoma, diabetic retinopathy, and myopia.
In a light-induced retinal degeneration (LIRD) model, exposure to bright light (10,000 lux) induces degeneration of photoreceptor cells in the retina9. Representative SD-OCT images reveal a thinner outer nuclear layer, which contains the photoreceptor cell bodies, in retinas from LIRD BALB/c mice compared with undamaged (control) mice (Figure 3A&3B). After quantifying the retinal layer thickness, a significant difference between undamaged and LIRD mice was observed for total retinal thickness (Figure 3C), outer nuclear layer thickness (Figure 3D), and IS/OS thickness (Figure 3E).
To experimentally model glaucomatous damage, we used a model of ocular hypertension (OHT)10. In brief, Brown Norway rats (n=35) received an injection of hypertonic saline into the limbus vein of one eye while the contralateral eye served as an internal control11. For glaucoma studies, we quantified retinal nerve fiber layer (RNFL) thickness. After 8 weeks of OHT, we observed distinct remodeling at the optic nerve head, including optic nerve cupping (Figure 4A&B). We then quantified RNFL thickness and found RNFL thinning after 8 weeks of OHT compared to baseline measurements (Figure 4C).
To model diabetic retinopathy, Goto-Kakizaki rats, a non-obese, polygenic model of diabetes that develops hyperglycemia as early as 2-3 weeks of age, were used12,13. Retinas from Goto-Kakizaki rats and Wistar rats (non-diabetic controls) were imaged using SD-OCT (Figure 5A&5B). At 6 weeks of age, RNFL and total retinal thickness were reduced in Goto-Kakizaki rats compared with Wistar rats in the central retina (data not shown) and the peripheral retina (Figure 5C&5D). The greatest differences were observed in the inferior and temporal quadrants of the retina (Figure 5C&5D).
To evaluate mouse models for myopia, axial length was measured in Bmal1-/- mice. Bmal1 is a clock gene of interest because circadian rhythms may play a role in myopia development14,15. The axial length of the Bmal1-/- mouse eye (Figure 6B) is visibly longer than the wild-type eye (Figure 6A) in the OCT images. Quantification of the axial length confirms that Bmal1-/- mice have significantly longer axial lengths at 84 days of age (Figure 6C), showing that the lack of the clock gene contributes to myopia development.
This protocol generated images of ocular structures in models of retinal degeneration, glaucoma, diabetic retinopathy, and myopia. Images were of sufficient quality such that ocular dimensions, including outer nuclear layer, retinal nerve fiber layer, total retinal thickness, and axial length, could be quantified. The results showed that significant differences in the dimensions of ocular structures could be observed in vivo using SD-OCT.
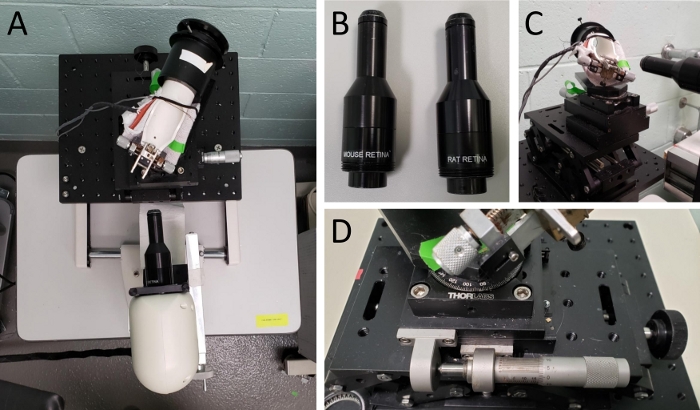
Figure 1: Setup of SD-OCT equipment.
(A) Picture of rodent alignment system and OCT scan head. (B) Picture of rat and mouse OCT lenses. (C) Picture of mouse rodent alignment system illustrating its ability to move in 3-dimensional space. (D) Close up of the rodent alignment system, specifically the knobs that control its movement. Please click here to view a larger version of this figure.
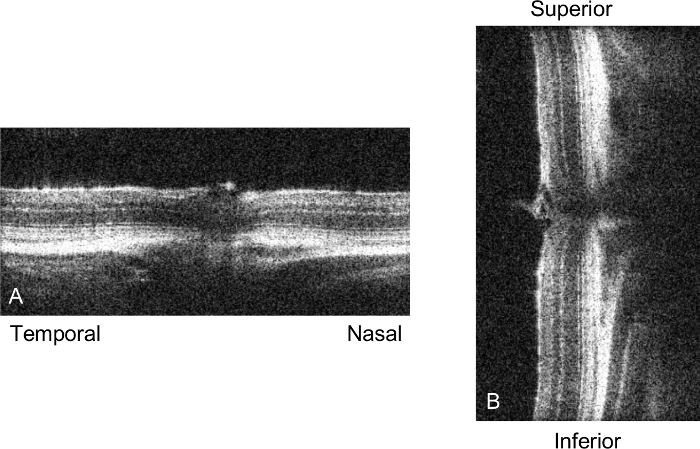
Figure 2: SD-OCT sample scan.
Picture of a live scan of the mouse retina just prior to taking a volume or radial scan. (A) depicts the nasal-temporal alignment, while (B) shows the superior-inferior alignment. Once the retinas in these two images are straight in their respective vertical or horizontal planes and the optic nerve is centered in both images, we proceed to acquire the SD-OCT image. Please click here to view a larger version of this figure.
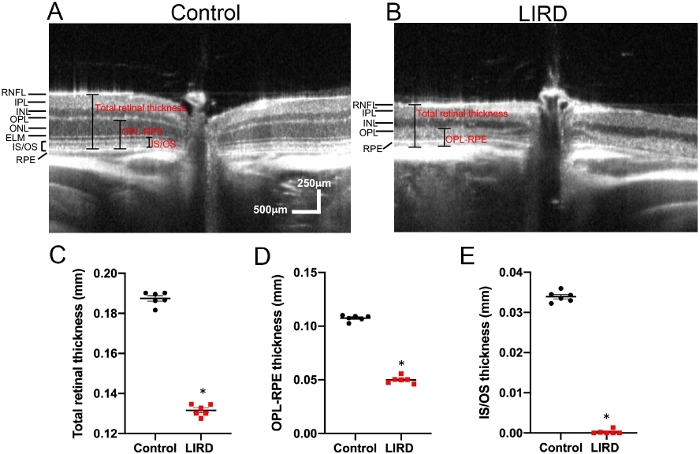
Figure 3: Using SD-OCT to track thinning of the photoreceptor layer over time in a mouse model of retinal degeneration.
(A) Representative SD-OCT scan of an undamaged (control) retina from a BALB/c mouse. (B) Representative SD-OCT scan of a retina from a light-induced retinal degeneration (LIRD) BALB/c mouse. (C-E) Quantification of total retinal thickness (C), outer nuclear layer (ONL) thickness (D), and inner segment/outer segment (IS/OS) thickness (E) in undamaged and LIRD Balb/c mice. Mean ± SEM. Please click here to view a larger version of this figure.
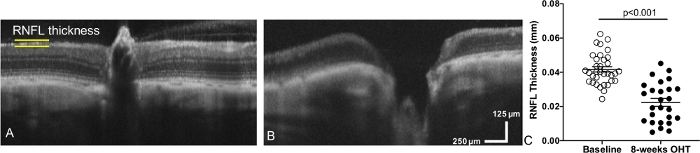
Figure 4: Using SD-OCT we measured a decrease in retinal nerve fiber layer thickness and observed optic nerve cupping after inducing ocular hypertension in a rat model of glaucoma.
(A) Representative SD-OCT scan of a retina and optic nerve head from a rat eye taken prior to inducing ocular hypertension (Baseline: OHT). (B) SD-OCT scan of the same rat retina after 8-weeks of OHT (experimental model of glaucoma). (C) Quantification of retinal nerve fiber layer (RNFL) thickness at baseline compared to OHT eyes. Mean ± SEM. This data has been modified from Feola et al.11 Please click here to view a larger version of this figure.
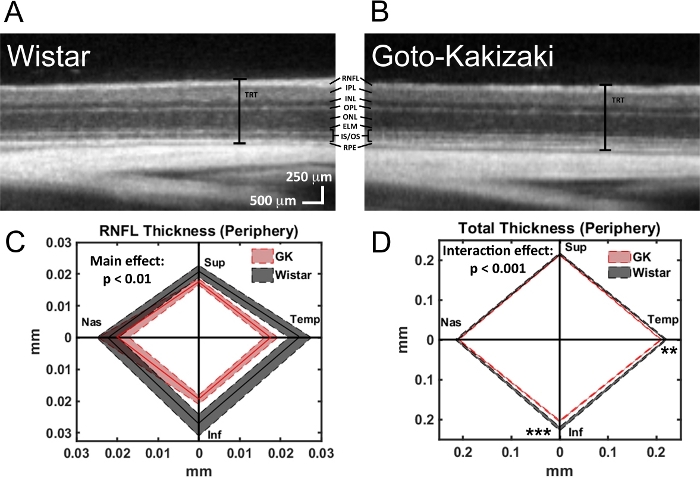
Figure 5: Using SD-OCT to observe decreased total retinal thickness as well as decreased thickness of specific retinal layers in a rat model of diabetes.
(A) Representative SD-OCT scan of a retina from a Wistar (Wild-type control) rat. (B) Representative SD-OCT scan of a retina from a Goto-Kakizaki (diabetic) rat. Retinal layers: retinal nerve fiber layer (RNFL), inner plexiform layer (IPL), inner nuclear layer (INL), outer plexiform layer (OPL), outer nuclear layer (ONL), external limiting membrane (ELM), inner segments/outer segments (IS/OS), retinal pigment epithelium (RPE), and total retinal thickness (TRT). (C-D) Quantification of RNFL (C) and total retinal thickness (D) in Wistar and Goto-Kakizaki retinas where the central line is the mean and the shaded area is the SEM for all four quadrants (Sup, Superior; Temp, Temporal; Inf, Inferior; Nas, Nasal) of the peripheral retina (1.2 mm from the optic nerve head). ** p < 0.01, *** p < 0.001. This figure has been modified from Allen et al.13 Please click here to view a larger version of this figure.
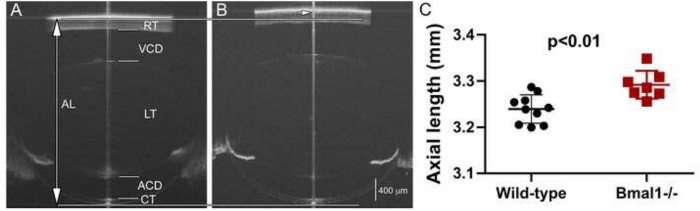
Figure 6: Using SD-OCT to evaluate axial length in a mouse model of myopia.
Whole eye SD-OCT images of wild-type (A) and Bmal1-/- (B) mouse eyes at 84 days of age. The eyes of Bmal1-/- mice have significantly longer axial length than the wild-type eyes (C). AL: axial length; RT: retinal thickness; VCD: vitreous chamber depth; LT: lens thickness; ACD: anterior chamber depth; CT: corneal thickness. The long vertical line indicates axial length boundaries (top and bottom indicated by horizontal line) for the wild-type eye. Short arrow indicates the posterior axial length marking for the Bmal1-/- eye. Mean ± SEM. The central line down the middle of each image (A&B) is a vertical saturation artifact. It is typically used as a guide to center the eye, but if the scan is well aligned, it can be made to disappear. Please click here to view a larger version of this figure.
