In this study, we randomly divided 45 mice into three groups, the sham, the silk suture group, and the absorbable suture group (the number of each group on D0 (baseline), D14, and D28 after TAC was 15, 10, and 5, respectively). On D7, D14, D21, and D28 after the surgery, the constricted peak velocity was determined by echocardiography. We found that the blood flow velocity at the constriction was still greater than 3,000 mm/s in the second week after TAC even though an absorbable suture had been used to constrict the aortic arch (Figure 1A). Moreover, the pressure gradient at the constriction of the absorbable suture group was maintained above 40 mmHg in 2 weeks (Figure 1B). Interestingly, there was no constriction in the fourth week after the surgery, indicating that the absorbable suture had been completely absorbed.
We also found that the left ventricular posterior wall thickness at end-diastole increased and left ventricular internal diameter at end-diastole decreased slightly on D14 after TAC (Figure 2A-C). It is interesting that the left ventricular posterior wall thickness at end-diastole in the absorbable suture group regressed substantially on D28 after TAC, which had no significant difference from the baseline level. In addition, the use of absorbable suture to make the model did not affect the ejection fraction of the left ventricle (Figure 2D).
HW / BW ratios of the silk suture group and the absorbable suture group had increased by 30% compared to the sham group. On D28 after TAC, myocardial hypertrophy regressed and the ratio fell back to the baseline level (Figure 3A) in the absorbable suture group, while the ratio increased by 64% in the silk suture group. The results of H&E staining also supported cardiac hypertrophy (Figure 3B). In conclusion, absorbable suture was suitable to cause transient pathological hypertrophy stimulation, which met the requirements of the myocardial hypertrophic preconditioning model.
Quantitative data has been presented as the mean ± SD. Comparisons among the sham, the silk suture, and the absorbable suture were performed using one-way ANOVA followed by Bonferroni’s post-hoc.
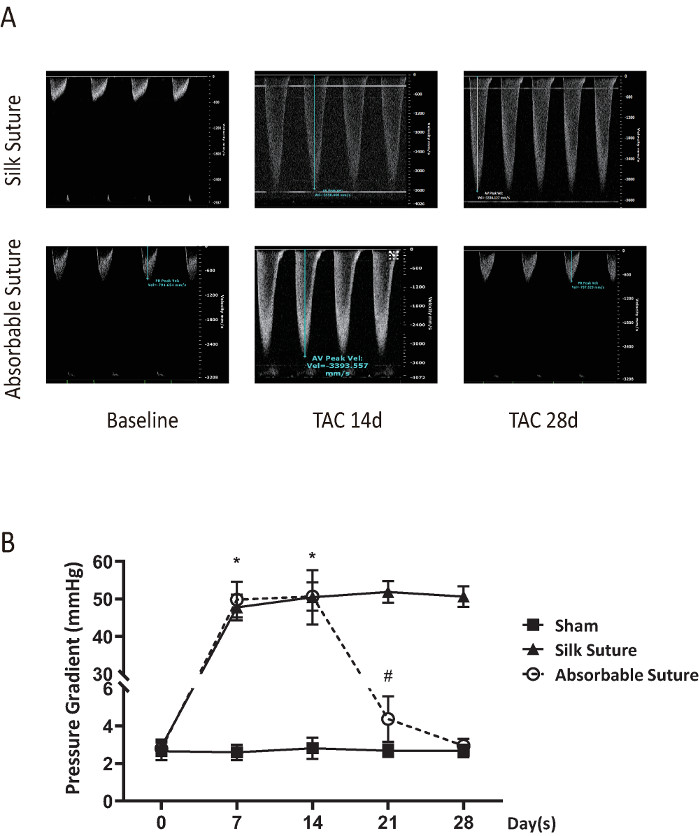
Figure 1: Pulsed-wave Doppler imaging and results from peak velocity and pressure gradient of the constriction. On D0 (baseline), D7, D14, D21, and D28 after TAC using silk suture or absorbable suture, aortic arch or the constriction was measured by a pulsed-wave Doppler. (A) Representative imaging of peak velocity on D0 (baseline), D14, and D28 after surgery in the silk suture group and the absorbable suture group. The blood flow velocity of the absorbable suture group returned to baseline while the velocity of the silk suture group was still greater than 3,000 mm/s on D28 after surgery. (B) The pressure gradient was calculated according to the modified Bernoulli's equation: pressure gradient = 4 x Vmax2 (V= maximum peak velocity). *: p < 0.05 vs sham. #: p < 0.05 vs the silk suture group (the number of each group on D0 (baseline), D14, and D28 after TAC was 15, 10, and 5, respectively). Data presented as mean ± SD. Please click here to view a larger version of this figure.
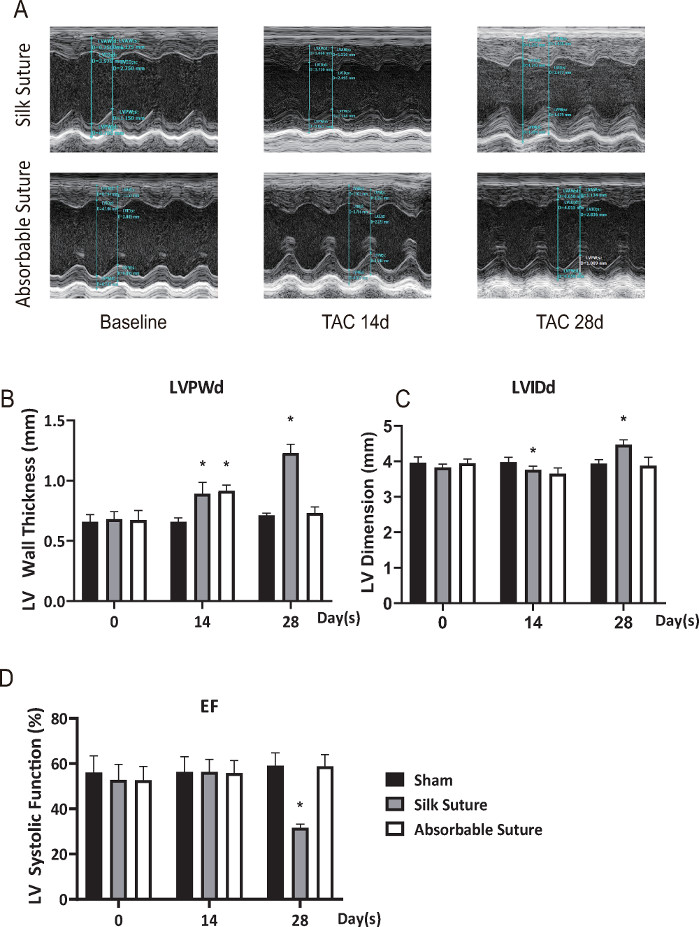
Figure 2: Left ventricular parameters of structure and systolic function. (A) M-mode imaging from the left ventricle (LV) in the silk suture group and the absorbable suture group on D0 (baseline), D14, and D28 after TAC. The representative image of LV wall thickness at end-diastole was about 0.70 mm (D0) to 1.089 mm (D28) in the silk suture group. As for the absorbable suture group, the wall thickness was about 0.658 mm (D28), which returned almost to the baseline. (B) Left ventricular posterior wall thickness at end-diastole (LVPWd). (C) Left ventricular internal diameter at end-diastole (LVIDd). (D) Left ventricular ejection fraction (EF). *: p < 0.05 vs the sham at the same time (the number of each group on D0 (baseline), D14, and D28 after TAC was 15, 10, and 5, respectively). Data presented as mean ± SD. Please click here to view a larger version of this figure.
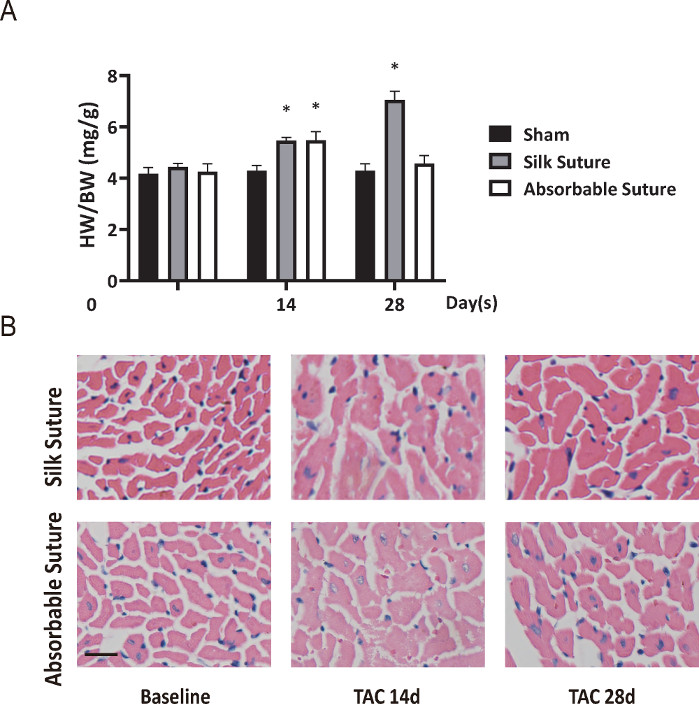
Figure 3: Reversible cardiac hypertrophy in the model of myocardial hypertrophic preconditioning. (A) Heart weight (HW) to body weight (BW) ratio. (B) Histological slices of heart stained with H&E (scale bar = 50 μm). Cardiomyocytes in the silk suture group were significantly enlarged from D14 to D28 while the size of cells mostly regressed on D28 in the absorbable suture group. *: p < 0.05 vs the sham at the same time (the number of each group on D0 (baseline), D14, and D28 after TAC was 15, 10, and 5, respectively). Data presented as mean ± SD. Please click here to view a larger version of this figure.
