The published results of FLA are shown in Table 2. A variety of methods and technologies are included. More than 400 patients who have undergone various forms of FLA for treatment of PCa are found within the SEER database.25 To quantify the number and characteristics of FLA reported in the literature we performed a systematic review of Medline and the Cochrane Library. Our search was performed using whole-field search terms including "focal laser ablation" and "prostate cancer." In total, 247 titles and abstracts were reviewed. Only cases reporting focal laser ablation, MRI, and oncologic outcomes were included. 13 peer-reviewed publications qualified for inclusion, representing 333 total patients (Table 1).
Treatment was performed with a 980 nm diode laser in all but 2 studies.26, 27 Treatment parameters consisted of power levels between 6 – 18 Watts and treatment times spanning 1 – 4 minutes per ablation site (Table 1). Treatment temperature monitoring was supplied by MRI thermometry in 9 studies and by direct temperature probe measurements in 3 studies (Table 1). All studies were performed in-bore, except those by Lindner and the later study by Natarajan.20, 26, 27
Median baseline PSA for the cohort was 5.7 (range 1.1 – 14.8). Following FLA, median PSA at 3, 6, 12 and 24 months was 3.9, 5.5, 3.8, and 3.9 respectively. Median baseline IPSS for the cohort was 6. Following FLA, median IPSS at 3, 6, 12 and 24 months was 5, 5.5, 7.3 and 11.5 respectively. Median baseline SHIM for the cohort was 20. Following FLA, median SHIM at 3, 6, 12 and 24 months was 19, 18, 20, and 19 respectively.
Across all studies, complications were inconsistently reported; however there was only one complication classified by the authors as Grade III (a urinary tract infection).16 The authors did not specify the features that classified this as a grade III event. Two recto-urethral fistulas, both closing spontaneously after prolonged catheterization,16 were reported as grade II adverse events.
Oncologic follow up was grouped by follow-up period: less than 6 months, one year, and two years (Table 2). Follow up biopsy was performed by MRI guided in-bore biopsy in 4 studies, and MRI-US fusion biopsy in 6 studies. Two studies utilized systematic biopsy and two studies performed 'treat-and-resect' investigations where the prostatectomy specimen was evaluated. Treatment success was defined according to a Delphi consensus protocol.28 In-field success was defined as the absence of ≥ GG2 PCa within the prior ablation site. Out of field failure was defines as ≥ GG2 outside the area of prior ablation. Among patients with follow up biopsy results, overall in-field success following treatment at 6 months (N=83), 1 year (N=64) and 2 years (N=39) was 83%, 83%, and 59% respectively (Table 2).
At UCLA, FLA of the prostate has been performed in three successive clinical trials starting in 2014.29–31 18 men with intermediate risk prostate cancer have undergone FLA, eight in-bore and 10 in clinic, without any grade III adverse events. Currently, an additional 10 men are undergoing FLA using the demonstrated device.31 All patients were evaluated before FLA with a 3T MRI (body coil), and MRI-US fusion biopsy with sampling from the ROI and systematic biopsy within 6 months of treatment. Both baseline and follow up biopsies were performed under MRI/US fusion guidance using the Artemis fusion system with tracking of all biopsy sites.
Table 1. Reported studies of focal laser ablation.
| Reference Number | Autore | Year | N | Median Age (Range) | Laser Power | Rx Time (sec) | Planned Margin | In-Bore Procedure | Temperature Monitoring | Baseline Gleason | ||||
| 3+3 | 3+4 | 4+3 | 4+4 | |||||||||||
| 26 | Lindner | 2009 | 12 | 56.5 (51-52) | – | 120 | – | No | Temperature probe | 12 | 0 | 0 | 0 | |
| 27 | Lindner | 2010 | 4 | 66 (61-73) | – | 120 | – | No | Temperature probe | 2 | 0 | 1 | 1 | |
| 5 | Oto | 2013 | 9 | 61 (52-77) | 6 – 15 W | – | – | Yes | MRI Thermometry | 8 | 1 | 0 | 0 | |
| 12 | Lee | 2014 | 23 | – | 8 W | 30-60 | – | Yes | MRI Thermometry | – | – | – | – | |
| 6 | Lepor | 2015 | 25 | 66 (49-84) | – | – | – | Yes | MRI Thermometry | 11 | 13 | 1 | 0 | |
| 18 | Al Barqawi | 2015 | 7 | 61 (56-69) | – | 90 | – | Yes | MRI Thermometry | 7 | 0 | 0 | 0 | |
| 15 | Bomers | 2016 | 5 | 66 (58-70) | – | – | 9 mm | Yes | MRI Thermometry | 2 | 2 | 1 | 0 | |
| 14 | Eggener | 2016 | 27 | 62 (-) | 6 – 15 W | 60-120 | 0 -7.5mm | Yes | MRI Thermometry | 23 | 3 | 1 | 0 | |
| 19 | Natarajan | 2016 | 8 | 63 (54-72) | 11 – 14 W | 180 | Custom* | Yes | Temperature probe # | 1 | 7 | 0 | 0 | |
| 20 | Natarajan | 2017 | 10 | 65 (52-74) | 13.75 W | 180 | Custom* | No | Temperature probe | 2 | 8 | 0 | 0 | |
| 35 | Chao | 2018 | 34 | 69 (52-88) | – | – | – | Yes | MRI Thermometry | 16 | 16 | 2 | 0 | |
| 17 | Al Hakeem | 2019 | 49 | 63 (51-73) | 10 – 15 W | 120 | 9 mm | Yes | MRI Thermometry | 13 | 29 | 7 | 0 | |
| 16 | Walser | 2019 | 120 | 60 (45-86) | 17 – 18 W | 180-240 | 5 mm | Yes | MRI Thermometry | 37 | 56 | 27 | 0 | |
Table 1: Dash (-) indicates information not available within the published manuscript. * indicates each margin was planned individually. # indicates monitoring was performed with both a temperature probe and MRI thermometry.
Table 2. Outcomes of focal laser ablation.
| Reference Number | First Author | Follow Up Biopsy Method | Follow up Biopsy | ≤ 6 Months | 12 Months | 24 Months | Adverse Events | ||||||
| Success | Failure | Success | Failure | Success | Failure | I | II | III | |||||
| 26 | Lindner | MRI Guided Bx | 12 | 12 | 0 | – | – | – | – | 2 | 0 | 0 | |
| 27 | Lindner | Prostatectomy | 4 | 2 | 2 | – | – | – | – | – | – | – | |
| 5 | Oto | MRI/US Bx | 9 | 9 | 0 | – | – | – | – | 1 | 1 | 0 | |
| 12 | Lee | MRI/US Bx | 13 | – | – | 12 | 1 | – | – | – | – | – | |
| 6 | Lepor | MRI Guided Bx | 21 | 20 | 1 | – | – | – | – | 0 | 0 | 0 | |
| 18 | Al Barqawi | Systematic Bx | 5 | – | – | 5 | 00 | – | – | – | 1 | 0 | |
| 15 | Bomers | Prostatectomy | 5 | 1 | 4 | – | – | – | – | – | – | – | |
| 14 | Eggener | MRI Guided Bx # | 27 | 27 | – | 7 | 31 | – | – | 7 | 2 | 0 | |
| 19 | Natarajan | MRI/US Bx | 8 | 6 | 53 | – | – | – | – | 23 | 7 | 0 | |
| 20 | Natarajan | MRI/US Bx | 10 | 6 | 40 | – | – | – | – | 38 | 6 | 0 | |
| 35 | Chao | MRI/US Bx | 22 | – | – | – | – | 13 | 9 | – | – | – | |
| 17 | Al Hakeem | MRI/US Bx | 49 | – | – | 40 | 91 | – | – | 34 | 11 | 0 | |
| 16 | Walser | MRI Guided Bx | 44* | – | – | – | – | 26 | 18 | 8 | 8 | 1 | |
Footnotes Table 2. Success = absence of ≥ GG2 prostate cancer within the ablation zone. Failure = presence of ≥ GG2 prostate cancer: total and out-of-field (subscript number). # indicates MRI guided biopsy was used for 6 months biopsy but only systematic biopsy was used for 12-month biopsy. * indicates that only patients with a PSA reduction of < 50% and positive post ablation MRI underwent biopsy; 76 patients did not undergo biopsy.

Figure 1: Treatment Planning and Assessment, shown via overlays on transverse MRI (top row) and in 3D (bottom row). Column A shows the delineation of treatment margins, which are expanded around the cancer-positive MRI target and bounded by nearby negative systematic biopsy cores (blue). Column B shows planning of ablation locations such that the treatment margins are overlapped to prevent 'skip' areas. Column C shows perfusion-weighted imaging collected 2 hours post-treatment, demonstrating correspondence between the planned and observed ablation extent. Please click here to view a larger version of this figure.
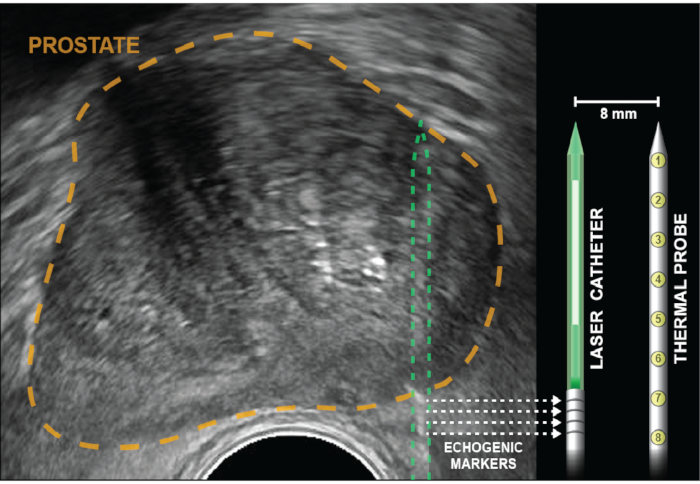
Figure 2: Axial ultrasound with prostate outlined in gold. Corner cube reflectors (echogenic bands), indicated by dotted arrows, are etched into the laser catheter 5 mm from the diffuser (white). Temperature probe is inserted to the same depth as the laser fiber, then locked into place and remains parallel to the laser 8 mm apart, out of the US plane of view. Eight thermal sensors, which are within the probe 4 mm apart, provide temperature recordings at points from the base of the echogenic bands to the tip of the laser catheter. Temperature measurements closest to the rectal wall are provided by thermal measurements at the base of the temperature probe (positions 6-8). Please click here to view a larger version of this figure.
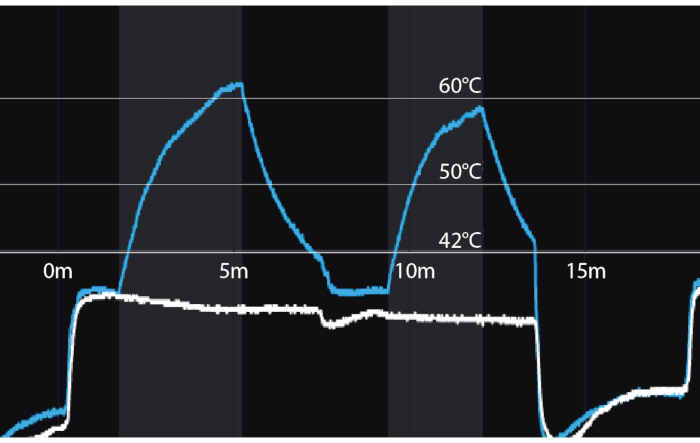
Figure 3: Temperature recordings during focal laser ablation for two successive ablations. Y-axis = temperature in Celsius. X-axis = time in minutes. Vertical shaded bars = periods of laser activation. Blue line = temperature 8mm from tip of laser fiber (distal thermocouple). White line = temperature 8 mm from proximal thermocouple nearest the rectal wall. A temperature of 60 degrees Celsius, achieved even briefly, assures coagulation necrosis. Please click here to view a larger version of this figure.
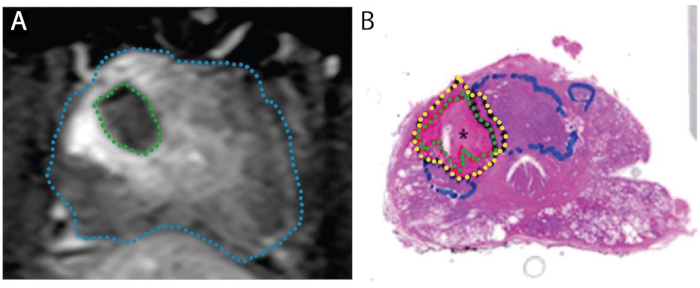
Figure 4: Images demonstrating concordance of ablation zone on post-treatment MRI (A) with actual necrotic zone on whole-mount specimen (B). Patient is 67-year-old male with PCa in right transition zone, Gleason score 3 + 4 = 7, participating in a 'treat and resect' trial. A. Post-ablation axial T1-weighted contrast-enhanced image, showing perfusion defect caused by laser treatment (green). B. Whole-mount H&E stain of the prostate. The necrotic tissue is delineated in green, the peri-necrotic tissue in yellow, and intact tumor (untreated) in blue. Reproduced under a Creative Commons license from Bomers et al, World Journal of Urology.15 Please click here to view a larger version of this figure.
