Although conventional T cells form the main repertoire of adaptive immune response against viral infection to facilitate viral clearance, the innate T cell population works across a broader spectrum to suppress the viral load for effective clearance at a later stage. Therefore, this protocol specifically creates a robust condition to study innate T cells, their activation, and their functional population following influenza infection, without needing epithelial and immune cell samples from the same donor. This protocol can also be applied to other viruses, although it may be limited to viruses with apical release, i.e., no virus should enter the basal layer to come into contact with the PBMC compartment.
Based on the representative results in Figure 1, this protocol can help to obtain hNESPC populations grown from a primary cell suspension in a 3T3 feeder layer. Figure 1 provides a sample of the expected progression of the hNESPCs as they grow on the 3T3 feeder layer. These cells will be used for differentiation in the ALI culture to obtain multilayered hNECs, complete with functional ciliated and goblet cells (Figure 4). Using the hNECs, innate T-cell activation can be investigated using flow cytometry. The results shown in Figure 5 show the detection of MAIT cell, γδ-T cell, and NK cell populations, which were significantly increased in co-culture involving hNECs infected with influenza virus. This setup can then be applied to other strains of the influenza virus to tease out the universal population across strains, as well as other viruses and their ability to activate innate T cell populations. In addition, the detection panel can also be customized according to the innate immune cell population of interest to observe their respective activation under co-culture conditions with infected epithelial cells.
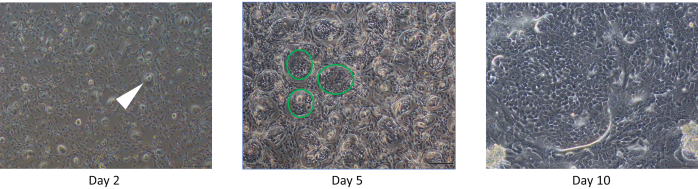
Figure 1: hNESPCs grown on a 3T3 feeder layer 2/5/10 days from seeding. Day 2: Note the islets of hNESPCs (an example is demarcated with a white arrow) that should be observed 2 days after seeding on the 3T3 feeder layer. Day 5: The islets observed on Day 2 should now be larger (examples of islands of hNESPCs are demarcated by green circles), and the 3T3 layer should be observed to be degenerating. Day 10: The hNECPSs should be dominating the entire plate with little or no 3T3 cells visible. Scale bars for Day 2 and Day 5 = 50 µm based on a magnification of 200x, scale bar for Day 10 = 100 µm based on a magnification of 100x. Abbreviation: hNESPCs = human nasal epithelium stem/progenitor cells. Please click here to view a larger version of this figure.
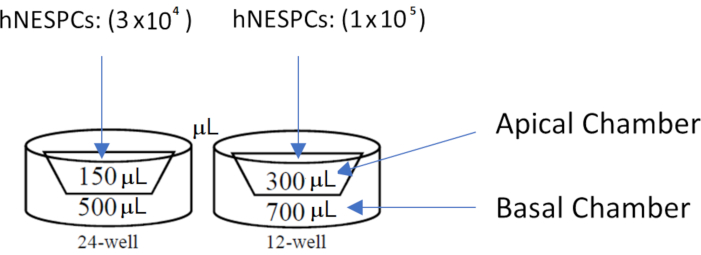
Figure 2: Well diagrams for membrane inserts in 24-well and 12-well plates. Note the medium volume to be used for each compartment. hNESPCs are seeded in the apical chambers of the membrane inserts. Abbreviation: hNESPCs = human nasal epithelium stem/progenitor cells. Please click here to view a larger version of this figure.
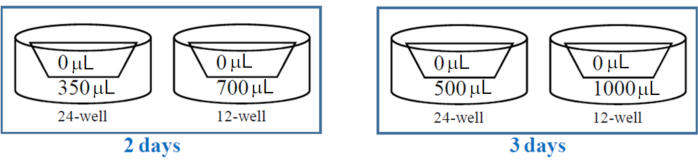
Figure 3: Well diagrams for membrane inserts in 24-well and 12-well plates for ALI co-culture establishment. Note the medium volume to be used for each compartment. Note the differences in medium volume to be used for the different intervals (2 days/3 days) between medium changes. Abbreviation: ALI = air-liquid interface. Please click here to view a larger version of this figure.
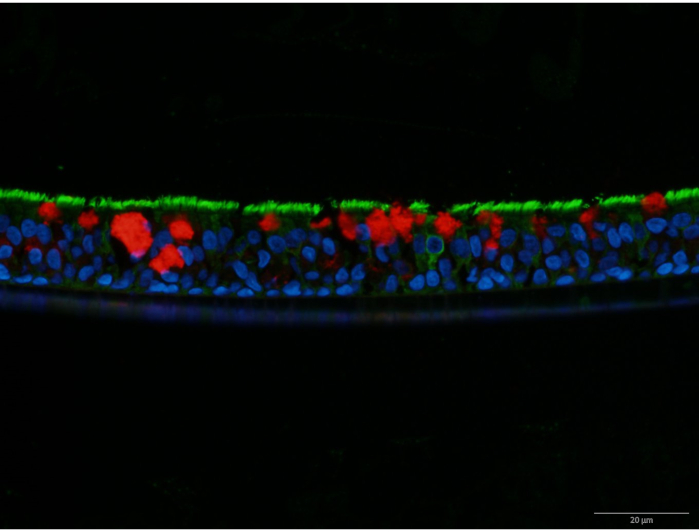
Figure 4: β4-Tubulin and MUC5AC co-stain of an hNEC layer. β4-Tubulin is stained in green, while MUC5AC is stained in red. The nuclei are stained in blue with DAPI. MUC5AC indicates the presence of mucus-producing goblet cells, while β4-tubulin indicates the presence of cilia on ciliated cells. Scale bar = 20 µm based on 600x magnification. Abbreviations: hNEC = human nasal epithelial cell; MUC5AC = mucin 5AC; DAPI = 4′,6-diamidino-2-phenylindole. Please click here to view a larger version of this figure.
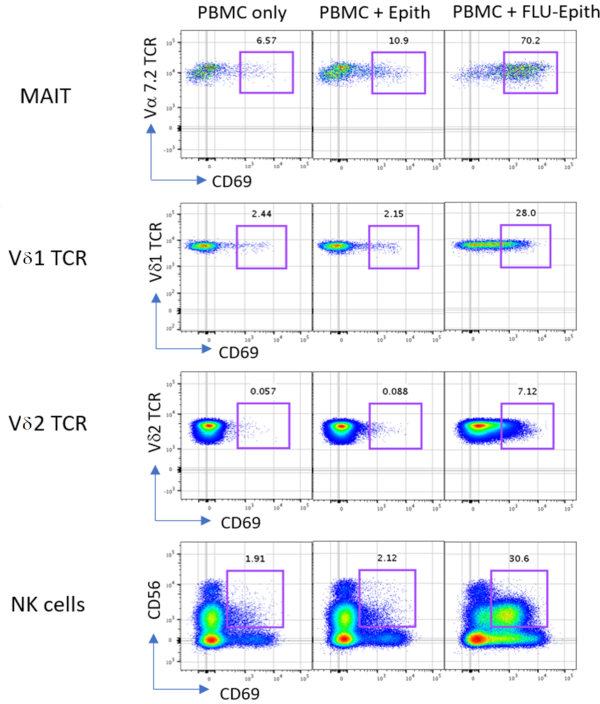
Figure 5: Representative results of PBMCs incubated with or without nasal epithelium or influenza-infected epithelium for 24 h. Activation of MAIT, Vδ1 T cells, Vδ2 T cells, and NK cells was determined by cell-type-specific markers including Vα 7.2 TCR, Vδ1 TCR, Vδ2 TCR, CD56, and CD69 staining. The values above the gates indicate the percentage of CD69-positive cells. Abbreviations: PBMCs = peripheral blood mononuclear cells; Epith = nasal epithelium; FLU-Epith = influenza-infected epithelium; MAIT = mucosal-associated invariant T cells; NK = natural killer; TCR = T-cell receptor; CD = cluster of differentiation. Please click here to view a larger version of this figure.
| Medium | Recipe | Composition | Comments |
| Medium 3 | DMEM/Nutrient Mixture F-12 | 500 mL | |
| Human Epithelial Growth Factor | 5 ng/mL | ||
| Insulin | 2.5 µg/mL | ||
| Cholera Toxin | 0.1 nM | ||
| Hydrocortisone | 0.5 µg/mL | ||
| 3,3',5-triiodo-l-thyronine | 2 nM | ||
| N-2 supplement | 5 mL | 10 µL/mL | |
| Antibiotic-Antimycotic | 5 mL | ||
| Differentiation Media | PneumaCult-ALI Basal Medium | 441 mL | |
| PneumaCult-ALI 10x Supplement | 50 mL | ||
| Hydrocortisone Solution (200x) | 2.5 mL | ||
| 0.2% (2 mg/mL; 1000 IU/mL) Heparin Sodium Salt in Phosphate-Buffered Saline | 1 mL | ||
| Antibiotic-Antimycotic (100x) | 5 mL | ||
| PneumaCult-ALI Maintenance Supplement (100x) | 500 µL | Only to be added right before use | |
| Complete Dulbecco's Minimal Essential Medium (DMEM) | DMEM/High Glucose | 450 mL | |
| Heat-inactivated Fetal Bovine Serum | 50 mL | ||
| Antibiotic-Antimycotic (100x) | 5 mL | ||
| Complete Roswell Park Memorial Institute (RPMI) Medium | RPMI 1640 (w L-Glutamine) | 445 mL | |
| Heat-inactivated Fetal Bovine Serum | 50 mL | ||
| Antibiotic-Antimycotic (100x) | 5 mL | ||
| Complete Eagle's Minimal Essential Medium (EMEM) | EMEM (w L-Glutamine) | 450 mL | |
| Heat-inactivated Fetal Bovine Serum | 50 mL | ||
| Infection Medium | EMEM (w L-Glutamine) | 4 mL | |
| TPCK Trypsin (500 µg/mL) | 8 µL | Final TPCK Trypsin Concentration of 1 µg/mL | |
| Magnetic-Activated Cell Sorting Buffer | 1x PBS | 498 mL | |
| 0.5 M EDTA | 2 mL | ||
| BSA (Tissue Culture Grade) | 2.5 g | ||
| Mitomycin C-Supplemented Complete DMEM | Complete DMEM | 10 mL | |
| Mitomycin C | 500 μL | Mitomycin C (10 µg/mL) |
Table 1: Recipe for media used.
| Cell surface marker | Fluorophore |
| Vδ1 T-cell receptor (TCR) | Fluorescein isothiocyanate (FITC) |
| Vδ2 TCR | Peridinin-cholorphyll-protein (PerCP) |
| CD3 | V500 |
| CD8 | Allophycocyanin-Cyanine 7 dye (APC-Cy7) |
| CD14 | Phycoerythrin (PE)-CF594 |
| CD56 | Phycoerythrin (PE)-Cyanine 7 (Cy7) |
| CD69 | Brilliant Violet 421 (BV421) |
| CD83 | Allophycocyanin (APC) |
| CD161 | Brilliant Violet 605 (BV605) |
| Vα 7.2 | Phycoerythrin (PE) |
| CD38 | Brilliant UltraViolet 395 (BUV395) |
Table 2: Sample surface staining markers.
| qPCR Reaction Mix | qPCR Master Mix | 5 µL |
| Nuclease-free Water | 3 µL | |
| Forward Primer (1 mM) | 0.5 µL | |
| Reverse Primer (1 mM) | 0.5 µL | |
| cDNA (12.5 ng/µL) | 1 µL | |
| Total Reaction Volume | 10 µL | |
| RT-PCR Reaction Mix | RT-PCR 5x Buffer | 2.5 µL |
| Random Primers (500 ng/µL) | 0.2 µL | |
| RNase Inhibitor | 0.625 µL | |
| dNTP Mix | 2.5 µL | |
| Reverse Transcriptase | 0.5 µL | |
| RNA (200 ng/µL) | 1 µL | |
| Nuclease-Free Water | 12.675 µL | |
| Total Reaction Volume | 20 µL |
Table 3: Recipe for reaction mixes of reverse-transcription polymerase chain reaction (RT-PCR) and quantitative PCR (qPCR).
