Cardiogene shock (CS) is een toestand van weefselhypoperfusie met of zonder gelijktijdige hypotensie, waarbij het hart niet in staat is om voldoende bloed en zuurstof te leveren om aan de eisen van het lichaam te voldoen, wat resulteert in orgaanfalen. Het is ingedeeld in stadia A tot E door de Society of Cardiovascular Angiography and Interventions (SCAI): stadium A – patiënten met een risico op CS; stadium B – patiënten in het beginstadium van CS met hypotensie of tachycardie zonder hypoperfusie; stadium C – klassiek CS met koud en nat fenotype dat inotropen / vasopressoren of mechanische ondersteuning vereist om de perfusie te behouden; fase D – verslechtering van de huidige medische of mechanische ondersteuning die escalatie naar meer geavanceerde apparaten vereist; en stadium E – omvat patiënten met circulatoire collaps en refractaire aritmieën die actief een hartstilstand ervaren met voortdurende cardiopulmonale reanimatie1. De meest voorkomende oorzaken van CS zijn acute MI (AMI) die 81% van de gevallen vertegenwoordigt in een recent gerapporteerde analyse2, en acuut gedecompenseerd hartfalen (ADHF). CS wordt klassiek gekenmerkt door congestie en verminderde perfusie, gemanifesteerd door verhoogde vuldrukken (pulmonale capillaire wigdruk [PCWP], linkerventrikel einddiastolische druk [LVEDP], centrale veneuze druk [CVP] en rechterventrikel einddiastolische druk [RVEDP]), verminderde cardiale output (CO), cardiale index (CI), cardiale output (CPO), cardiale output (CPO) en eindorgaanstoring3 . In het verleden waren de enige beschikbare behandelingen voor AMI gecompliceerd door CS vroege revascularisatie en medisch management met inotropen en / of vasopressoren4. Meer recent, met de komst van mechanische circulatoire ondersteuning (MCS) apparaten en de erkenning dat escalatie van vasopressoren geassocieerd is met verhoogde mortaliteit, is er een paradigmaverschuiving geweest in de behandeling van zowel AMI- als ADHF-gerelateerd CS5,6.
In het huidige tijdperk van percutane ventriculaire hulpmiddelen (pVAD) zijn er een aantal MCS-apparaatplatforms / configuraties beschikbaar, die univentriculaire of biventriculaire bloedsomloop- en ventriculaire ondersteuning bieden met en zonder oxygenatiecapaciteit7. Ondanks een gestage toename van het gebruik van pVAD’s voor de behandeling van zowel AMI als ADHF CS, zijn de sterftecijfers grotendeels onveranderd gebleven5. Met opkomend bewijs voor mogelijke klinische voordelen voor het vroegtijdig lossen van de linker ventrikel (LV) in AMI8 en vroeg gebruik van MCS in AMI CS9, blijft het gebruik van MCS toenemen.
Het MCS-apparaat Left Atrial to Femoral Artery Bypass (LAFAB) omzeilt de LV door bloed uit het linkeratrium (LA) af te voeren en via de dijbeenslagader terug te brengen naar de systemische arteriële circulatie (figuur 1). Het wordt ondersteund door een externe centrifugaalpomp die 2,5-5,0 liter per minuut (L / m) debiet biedt (nieuwe generatie pomp, aangeduid als LifeSPARC, geschikt voor maximaal 8 L / m debiet) afhankelijk van de grootte van de canules. Zodra het bloed uit de LA is geëxtraheerd via de transseptale veneuze canule, gaat het door de externe centrifugaalpomp die het bloed terugcirculeert in het lichaam van de patiënt via de arteriële canule die in de femorale slagader is geplaatst.
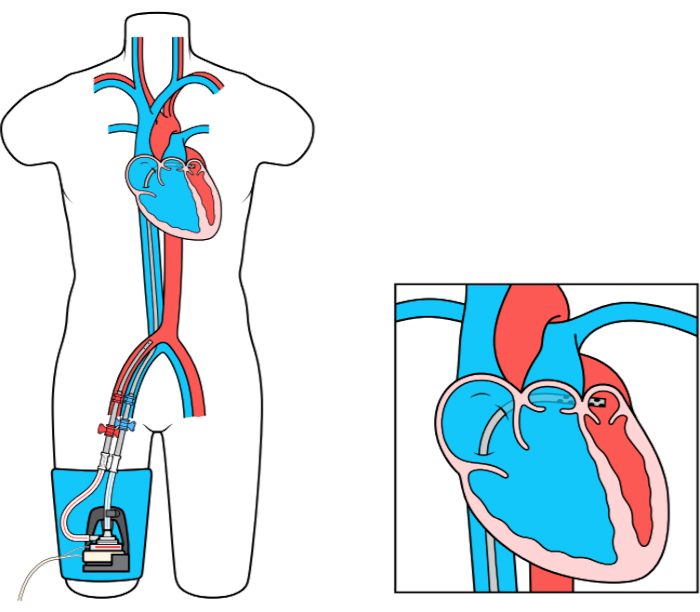
Figuur 1: LAFAB setup. Afbeelding met dank aan TandemLife, een volledige dochteronderneming van LivaNova US Inc. Klik hier om een grotere versie van dit cijfer te bekijken.
