Le choc cardiogénique (CS) est un état d’hypoperfusion tissulaire avec ou sans hypotension concomitante, dans lequel le cœur est incapable de fournir suffisamment de sang et d’oxygène pour répondre aux demandes du corps, entraînant une défaillance d’organe. Il est classé en stades A à E par la Society of Cardiovascular Angiography and Interventions (SCAI): stade A – patients à risque de CS; stade B – patients au stade précoce de la CS avec hypotension ou tachycardie sans hypoperfusion; stade C – CS classique avec phénotype froid et humide nécessitant des inotropes / vasopresseurs ou un soutien mécanique pour maintenir la perfusion; stade D – détérioration du support médical ou mécanique actuel nécessitant une escalade vers des dispositifs plus avancés; et stade E – comprend les patients présentant un collapsus circulatoire et des arythmies réfractaires qui subissent activement un arrêt cardiaque avec réanimation cardiorespiratoire en cours1. Les causes les plus courantes de CS sont l’IM aiguë (AMI) représentant 81 % des cas dans une analyse récemment rapportée2, et l’insuffisance cardiaque aiguë décompensée (ADHF). Le CS est classiquement caractérisé par une congestion et une altération de la perfusion, qui se manifestent par des pressions de remplissage élevées (pression de coin capillaire pulmonaire [PCWP], pression diastolique terminale ventriculaire gauche [LVEDP], pression veineuse centrale [CVP] et pression diastolique terminale ventriculaire droite [RVEDP]), diminution du débit cardiaque (CO), de l’indice cardiaque (IC), de la puissance cardiaque (CPO) et dysfonctionnement de l’organe final3 . Dans le passé, les seuls traitements disponibles pour l’AMI compliquée par la CS étaient la revascularisation précoce et la prise en charge médicale avec des inotropes et/ou des vasopresseurs4. Plus récemment, avec l’avènement des dispositifs de soutien circulatoire mécanique (MCS) et la reconnaissance que l’escalade des vasopresseurs est associée à une mortalité accrue, il y a eu un changement de paradigme dans le traitement de l’AMI et de l’ADHF CS5,6.
À l’ère actuelle des dispositifs d’assistance ventriculaire percutanée (pVAD), il existe un certain nombre de plates-formes /configurations de dispositifs MCS disponibles, qui fournissent un soutien circulatoire et ventriculaire univentriculaire ou biventriculaire avec et sans capacité d’oxygénation7. Malgré l’augmentation constante de l’utilisation des DAEP pour traiter à la fois l’AMI et l’ADHF CS, les taux de mortalité sont restés en grande partie inchangés5. Avec les nouvelles preuves des avantages cliniques possibles du déchargement précoce du ventricule gauche (LV) dans AMI8 et l’utilisation précoce de MCS dans AMI CS9, l’utilisation de MCS continue d’augmenter.
Le dispositif MCS LAFAB (Left Atrial to Femoral Artery Bypass) contourne le LV en drainant le sang de l’oreillette gauche (LA) et en le renvoyant dans la circulation artérielle systémique via l’artère fémorale (Figure 1). Il est soutenu par une pompe centrifuge externe qui offre un débit de 2,5 à 5,0 litres par minute (L / m) (pompe de nouvelle génération, désignée LifeSPARC, capable d’un débit allant jusqu’à 8 L / m) en fonction de la taille des canules. Une fois que le sang est extrait de l’AL via la canule veineuse transseptale, il passe à travers la pompe centrifuge externe qui recircule le sang dans le corps du patient via la canule artérielle placée dans l’artère fémorale.
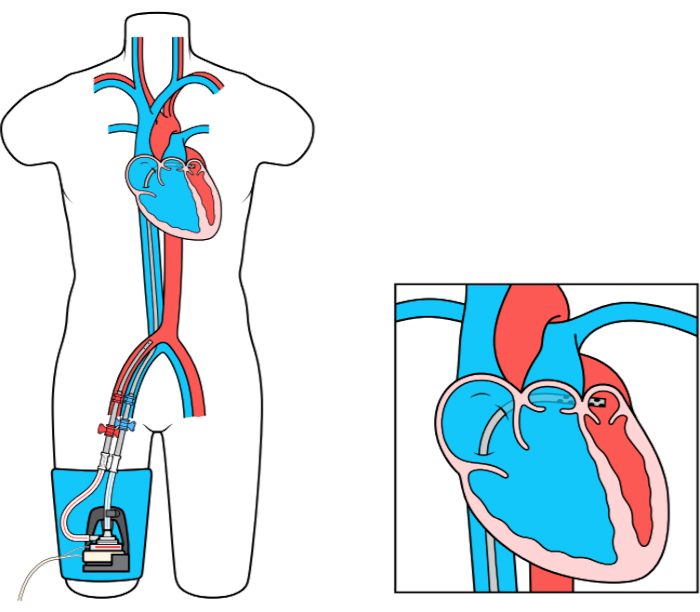
Figure 1 : configuration de LAFAB. Image reproduite avec l’aimable autorisation de TandemLife, une filiale en propriété exclusive de LivaNova US Inc. Veuillez cliquer ici pour voir une version agrandie de ce chiffre.
