הלם קרדיוגני (CS) הוא מצב של תת-לחץ דם של רקמות עם או בלי תת לחץ דם במקביל, שבו הלב אינו מסוגל לספק מספיק דם וחמצן כדי לענות על דרישות הגוף, וכתוצאה מכך אי ספיקת איברים. הוא מסווג לשלבים א’ עד ה’ על ידי האגודה לאנגיוגרפיה והתערבויות לב וכלי דם (SCAI): שלב A – חולים בסיכון למדעי העיתות; שלב B – חולים בשלב תחילת של CS עם תת לחץ דם או טכיקרדיה ללא hypoperfusion; שלב C – CS קלאסי עם פנוטיפ קר ורטוב הדורש inotropes / vasopressors או תמיכה מכנית כדי לשמור על זלוף; שלב D – הידרדרות בתמיכה הרפואית או המכנית הנוכחית הדורשת הסלמה למכשירים מתקדמים יותר; ושלב E – כולל חולים עם התמוטטות במחזור הדם והפרעות קצב עקשן אשר חווים באופן פעיל דום לב עם החייאה לבבית מתמשכת1. הגורמים הנפוצים ביותר למדעת המחשבים הם MI (AMI) חריף המייצג 81% מהמקרים בניתוח שדווח לאחרונה2, ואי ספיקת לב חריפה (ADHF). CS מאופיין קלאסית על ידי גודש זלוף לקוי, המתבטא בלחצי מילוי גבוהים (לחץ טריז נימי ריאתי [PCWP], לחץ קצה-דיאסטולי בחדר השמאלי [LVEDP], לחץ ורידי מרכזי [CVP], ולחץ קצה-דיאסטולי בחדר הימני [RVEDP]), ירידה בתפוקת הלב (CO), מדד הלב (CI), תפוקת כוח הלב (CPO) ותקלה באיבר הקצה3 . בעבר, הטיפולים הזמינים היחידים עבור AMI מסובך על ידי CS היו revascularization מוקדם וניהול רפואי עם inotropes ו /או vasopressors4. לאחרונה, עם הופעתם של מכשירי תמיכה מכניים במחזור הדם (MCS) וההכרה כי הסלמה של vasopressors קשורה לתמותה מוגברת, חל שינוי פרדיגמה בטיפול הן של AMI ו- ADHF הקשורים CS5,6.
בעידן הנוכחי של התקני סיוע חדרית מלתועים (pVAD), ישנן מספר פלטפורמות / תצורות התקן MCS זמינות, המספקות תמיכה במחזור הדם ובחיקונים חד-חדריים עם ובלי יכולת חמצון7. למרות עלייה מתמדת בשימוש ב-pVADs לטיפול הן ב-AMI והן ב-ADHF CS, שיעורי התמותה נותרו ברובם ללא שינוי5. עם ראיות המתעוררות ליתרונות קליניים אפשריים לפריקה מוקדמת של החדר השמאלי (LV) ב- AMI8 ושימוש מוקדם ב- MCS ב- AMI CS9, השימוש ב- MCS ממשיך לגדול.
התקן MCS של מפרזים שמאליים לעורק הירך (LAFAB) עוקף את ה-LV על ידי ניקוז דם מהאטריום השמאלי (LA) והחזרתו למחזור הדם המערכתי דרך עורק הירך (איור 1). הוא נתמך על ידי משאבה צנטריפוגלית חיצונית המציעה זרימה של 2.5-5.0 ליטר לדקה (L/m) (משאבת דור חדש, המיועדת ל- LifeSPARC, המסוגלת לזרימה של עד 8 ליטר/ מ’) בהתאם לגודל הקנולות. ברגע שהדם מופק מלוס אנג’לס דרך הצינורית הוורידית הטרנספטלית, הוא עובר דרך המשאבה הצנטריפוגלית החיצונית אשר מחזירה את הדם לגוף המטופל דרך הצינורית העורקית המונחת בעורק הירך.
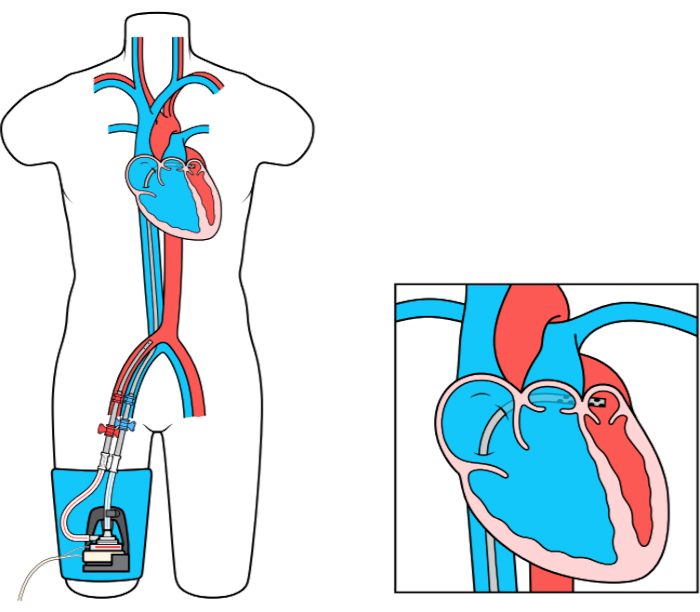
איור 1: הגדרת LAFAB. התמונה באדיבות TandemLife, חברת בת בבעלות מלאה של LivaNova US Inc. אנא לחץ כאן כדי להציג גרסה גדולה יותר של דמות זו.
