This protocol details a reliable means of inducing ischemia and tissue loss in the murine footpad using a combination of femoral artery and vein coagulation with L-NAME administration, a nitric oxide synthase inhibitor, in susceptible FVB mice. Figure 1 details the anatomy of the murine hindlimb vasculature and indicates the sites of the femoral artery and vein coagulation (yellow X), just proximal to the lateral circumflex femoral artery (LCFA) and proximal to the saphenopopliteal junction. The LCFA needs to be identified, and the coagulation sites respective to this structure are kept consistent throughout all surgical procedures. As described, 2 h before surgical procedures and on postoperative days 1-3, mice were also administered 40 mg/kg IP of L-NAME to maintain elevated tissue levels of oxidative stress. Figure 2 shows the variation in tissue loss that can be expected from this model one week after surgery, with Faber scores9 recorded in the lower right corner of each image.
DiI perfusion was performed in FVB mice at 5 and 20 days after femoral artery and vein coagulation to assess hindlimb reperfusion following induction of ischemia. Figure 3A illustrates the murine anatomy after dissection to expose the thoracic cavity. A butterfly needle is inserted into the left ventricle to begin cardiac perfusion. Note that the left ventricle appears slightly paler in color than the right ventricle. Figure 3B depicts the equipment set up with stopcocks connected in series and three syringes filled with PBS, DiI solution, and fixative. Following DiI perfusion, feet were harvested, skinned, and compressed between microscope slides as shown in Figure 3C,D before imaging with a confocal laser scanning microscope under 5x magnification. Reconstruction microscopy images revealed normal vascular anatomy in non-ligated control footpad (Figure 4A) compared with severely diminished perfusion to the footpad of ligated hindlimb 5 days after surgery (Figure 4B). Twenty days after surgery, perfusion to the footpad significantly improved (Figure 4C,D, and Figure 5B), although not to the extent of non-ligated control (Figure 4A and Figure 5A). Vascularity was quantified as described above using the Vessel Density plugin in Fiji. The vascular fraction for the control footpad was 28%. Five days after surgery, footpad vascular fraction was severely reduced to 2% but gradually recovered to 15% and 18% in two separate mice by 20 days postoperatively. To visualize the footpad vascular anatomy in 3D, we imported a stitched microscopy image into alternate image analysis and processing software to create a surface rendering as described previously (Supplementary Figure 1). A video of the surface rendering was then created using the animation functionality (Video 1).
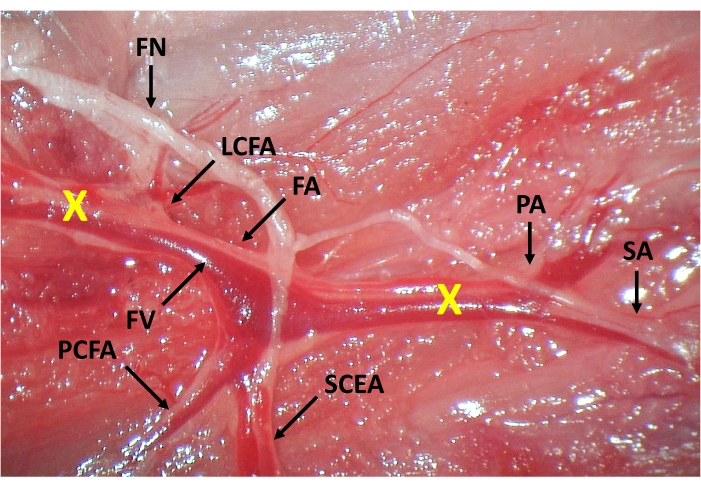
Figure 1: Anatomy of the murine hindlimb vasculature and sites of the femoral artery and vein coagulation. The external iliac artery continues as the femoral artery (FA) distal to the inguinal ligament. The first branches of the femoral artery include the lateral circumflex (LCFA) and deep femoral arteries (not pictured). More distally, the proximal caudal femoral (PCFA) and superficial caudal epigastric arteries (SCEA) branch from the FA proximal to the bifurcation of the saphenous (SA) and popliteal arteries (PA). The femoral nerve (FN) courses alongside the femoral vessels and should be gently isolated before coagulation of the femoral vessels. FA and femoral vein (FV) coagulation sites are also indicated (X). Please click here to view a larger version of this figure.
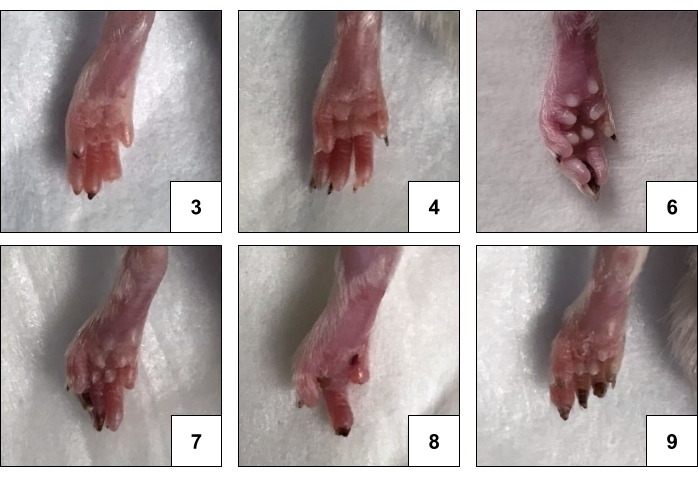
Figure 2: Representative images of hindlimb gangrene in FVB mice with corresponding Faber scores. The degree of ischemic changes induced by this model varies from one or more ischemic nails (Faber scores 1-5) to gangrenous digits (Faber scores 6-10) and partial or complete foot atrophy. Please click here to view a larger version of this figure.
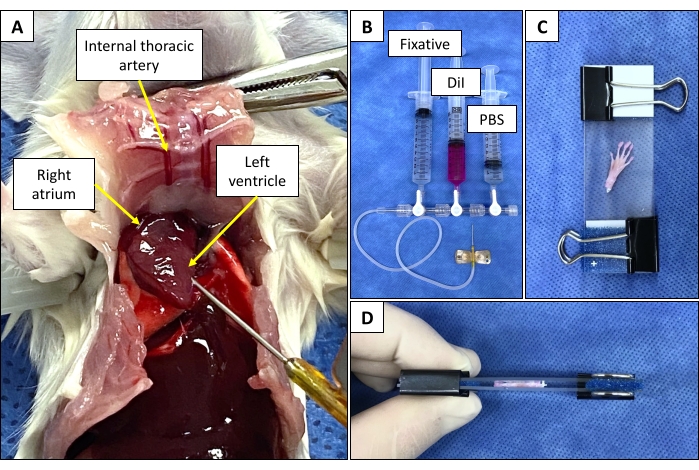
Figure 3: Animal dissection and equipment setup for DiI perfusion and mounting of mouse foot for imaging. (A) Anatomical photograph of the murine anatomy during DiI perfusion. The abdominal and the thoracic cavities are opened, the sternum is reflected, and the ribs are cut on either side of the sternum. A 25 G butterfly needle connected to the stopcock assembly is inserted into the left ventricle. (B) Three 3-way stopcocks are connected in series. Three 10 mL syringes are filled with fixative, DiI, and PBS and connected to the stopcock assembly. A 25 G butterfly needle is connected to the outflow port of the proximal stopcock. (C) Mounting skinned foot between two microscope slides with a folded foam biopsy pad and binder clip at each end to compress the slides together. (D) An alternative view of the skinned foot compressed between microscope slides. Please click here to view a larger version of this figure.
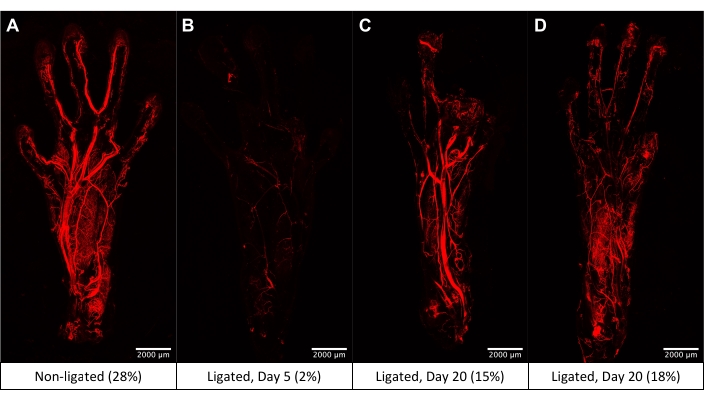
Figure 4: Representative 5x images obtained by confocal laser scanning microscopy of the mouse footpad following DiI perfusion with quantified vessel density expressed as a percent of ROI. (A) Normal footpad vasculature. (B) Footpad vasculature 5 days after femoral artery and vein coagulation shows severely reduced perfusion with minimal vessel opacification. (C) Footpad vasculature 20 days after femoral artery and vein coagulation demonstrates some reconstitution of distal flow to the metatarsal and digital arteries. (D) Image of an additional mouse footpad obtained 20 days after femoral artery and vein coagulation showing minimal large vessel compared to microvascular opacification. Please click here to view a larger version of this figure.
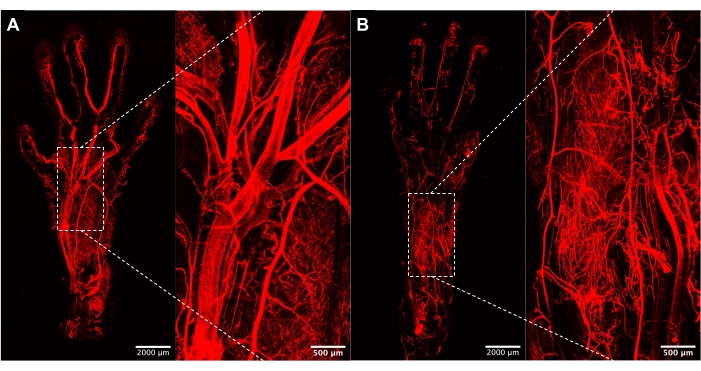
Figure 5: Magnified images of the footpad vasculature. (A) 5x and 20x images of control footpad vasculature demonstrating intact perfusion via the metatarsal and digital arteries. (B) 5x and 20x images of footpad from ligated hindlimb 20 days postoperatively showing reduced perfusion via larger metatarsal arterial branches but the development of an extensive, plush capillary network. Please click here to view a larger version of this figure.
Video 1: Animation of the 3D surface rendering of the footpad vasculature. Video displaying a surface rendering of the footpad vasculature illustrates the 3D resolution achievable with the described protocol. Please click here to download this Video.
Supplementary Figure 1: Steps in the surface rendering of DiI perfusion images. (A) Original DiI perfusion image imported into image analysis and processing software. (B) Surface rendering overlaid onto DiI perfusion image during setting of the threshold intensity. (C) Final 3D surface rendering of DiI perfusion microscopy image. Please click here to download this File.
