Solution injected into the subconjunctival space presents as a bleb depending on the injection volume.
In this experiment, 7 µL of AAV (7 × 109 viral genomes (vg)/eye) mixed with fluorescein at a final concentration of 0.1% was injected with a 36 G needle under a stereomicroscope, and the injection speed/pressure was held constant using a programmable syringe pump at 1 µL/s. A bleb can appear upon injection (arrow). A microscopic view of AAV vector administration to the murine SCJ compartment is shown in Figure 1.
Substances injected into the subconjunctival space diffuse around the globe of the eye and are distributed throughout the periocular tissues.
To define the distribution of AAV administered via SCJ injection, 7 µL of diluted India ink was injected into the subconjunctival space of a 10-month-old mouse after anesthetization. No bleeding, leakage, or backflow was detected during or following the SCJ injection. Thirty minutes post injection, the ocular and surrounding tissues were harvested and subsequently stained with Hematoxylin and Eosin (H&E) to visualize the distribution of India ink. The representative sagittal sections depicted in Figure 2 demonstrate that the dispersion of India ink occurred mainly adjacent to the extraocular muscles, in the outer surface of the sclera, and the periocular loose connective tissues (Figure 2).
Self-complementary AAV8 successfully transduces the cornea and periocular muscles following SCJ.
To determine the transduction profile of self-complementary AAV8 at eight weeks post injection, GFP abundance in whole-globe cross-sections was examined via immunofluorescence staining using an anti-GFP antibody at a dilution of 1:500. Images were taken under a fluorescence microscope (Figure 3). These results revealed that AAV vectors administered via SCJ injection efficiently transduce the periocular muscles posterior to the eye and the cornea.
Abundant vector genome and transgene expression in distinct eye compartments following SCJ injection
To quantitatively analyze the vector biodistribution and transgene expression, vector genome copy numbers in distinct eye compartments and organs such as the liver and heart were examined by qPCR (Figure 4A), while the transgene expression was tested by qRT-PCR (Figure 4B). These results suggest that SCJ injection of AAV8 results in transgene expression in the eyelid, conjunctiva, cornea, and optic nerve.
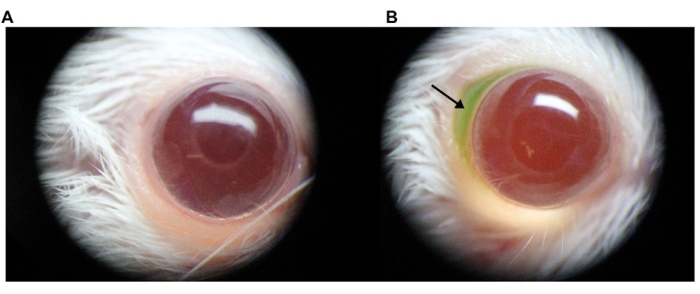
Figure 1: Microscopic view of AAV vector administration into the murine SCJ space. To allow for visualization of the formation of a bleb during the procedure, 1% fluorescein was directly added to the AAV vector preparation. Images were taken using a digital camera attached to a stereomicroscope. (A) Representative image of a noninjected eye; (B) representative image of an injected eye. The arrow indicates the injected AAV solution containing fluorescein in the SCJ space. Abbreviations: AAV = Adeno-associated virus; SCJ = subconjunctival. Please click here to view a larger version of this figure.
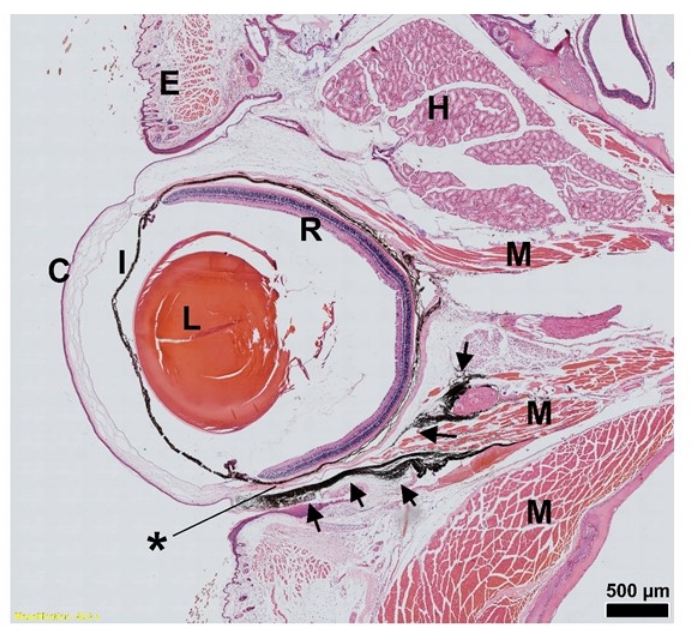
Figure 2: H&E staining of India ink distribution (arrow) after SCJ injection in the mouse eye. Sagittal sections of an eye injected with India ink are presented; 7 µL of India ink was injected at the indicated site. *, Injection site. Scale bar = 500 µm. Abbreviations: SCJ = subconjunctival; H&E = hematoxylin and eosin; C = cornea; I = iris; L = lens; R = Retina; E = eyelid; H = Harderian gland; M = muscle. Please click here to view a larger version of this figure.
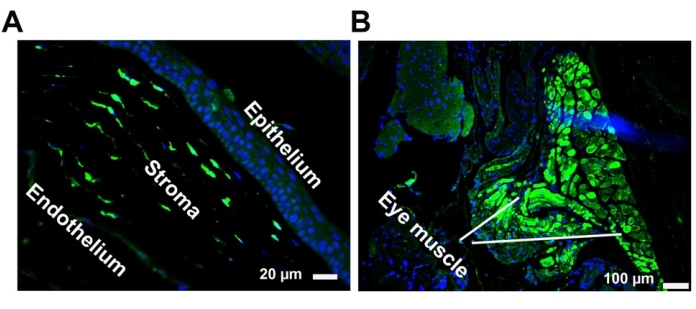
Figure 3: Representative GFP histology images of self-complementary AAV8 after SCJ injection. Transduction of the cornea (A) and eye muscles (B) following SCJ injection. GFP expression (green) was visualized via immunostaining in paraffin-embedded tissue sections with an anti-GFP antibody. Nuclei were stained with DAPI (blue). Scale bar = 100 µm (eye muscle), 20 µm (cornea). Abbreviations: GFP = green fluorescent protein; AAV = adeno-associated virus; SCJ = subconjunctival; DAPI = 4',6-diamidino-2-phenylindole. Please click here to view a larger version of this figure.
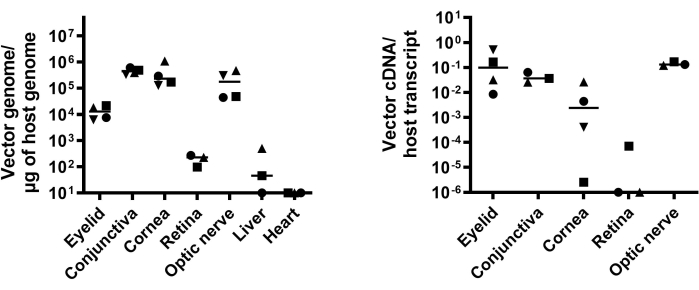
Figure 4: Quantitative analysis of vector biodistribution and transgene expression. (A) Vector biodistribution in eye compartments (eyelid, conjunctiva, cornea, optic nerve, and retina) and other organs (liver and heart) following SCJ is presented as vector genome copy number/µg of host genome DNA. (B) GFP abundance determined by qRT-PCR is presented as vector cDNA copy number/host transcript. This figure is modified from 13. Abbreviations: SCJ = subconjunctival; qRT-PCR = quantitative revere-transcription PCR; GFP =green fluorescent protein. Please click here to view a larger version of this figure.
