Diagnosis of underweight and parental infant-rearing abnormality
A pair of five-year-old common marmosets (Callithrix jacchus) obtained from a colony at Saitama Medical University gave birth to their first set of offspring (twins) overnight in May 2019. This was a spontaneous vaginal birth. Only one of the offspring (a male) was found alive and embracing the mother's body. Another sibling was found dead, the birth weight (less than 25 g) and sex unclear, multiple hours after death. The presence or absence of milk ingestion behavior between the mother and offspring was unknown at the first perinatal check.
The infant was weighed daily at approximately the same time. The delivery day weight was 26 g, lower than the standard15,16. The colony records of neonatal infants' weight for survival have a minimum weight of 27 g (Figure 2). The CRL was 9 cm. The father was frequently observed to be persistently licking the infant since day 1. Such paternal behavior has never been identified in our common marmoset colonies. By day 2, the infant lost weight (Figure 4, PD2(1), reaching the lowest weight 23 to 24 g recorded in our breeding history (the previous minimal record; 27 g), and did not appear to be initiating nursing. The infant did not appear to have the strength to initiate and maintain spontaneous suckling behavior.
Because of the condition of the infant, we searched for any evidence of abnormal parental rearing behavior in the recorded video. The father also showed strange behavior In addition to persistent licking, he appeared to be encouraging the infant to suckle his breast (see the accompanying video). The mother sometimes approached the father to touch the infant; however, the father appeared to brush the mother away, causing breastfeeding failure-milk duct closure and breast tautening followed by the mother's refusal to allow the infant to suckle because of pain. The mother's breast enlargement appeared painful and she seemed unwilling to be suckled, translating to "abandonment". This abnormal parental behavior was defined as "abuse" or "abandonment", behaviors that prevented the infant from feeding spontaneously. It was determined that intensive care was required.
Combination of formula and breast milk
Thus, the first feeding intervention (0.5 mL of formula by syringe) occurred at 10:30 h on postnatal day 2 (PD2) (Figure 4A). Fortunately, before further intervention, it was confirmed that the infant maintained both the rooting reflex (one of the most important neural functions at this neonatal stage) and the ability to cry loudly, producing the typical "Phee call"11,12,13. Two additional formula feedings were added at 12:30 h and 17:30 h during Day 2, resulting in a weight increase of 1 g to a body weight of 25 g.
Guided clinical care: voluntary participation in breastfeeding by mother and infant
On Day 2, breastfeeding intervention began. The mother was hand-held and her engorged breast was digitally massaged by the interventionist (Figure 4B). Next, the infant was placed on the mother's body and encouraged to spontaneously search for the nipple (Figure 4C). The mother maintained a tentative pose and showed limited resistance. The interventionist guided the mother to raise her arms to improve nipple access. During this process, the infant was confirmed to be feeding continuously. The mother showed some reluctance when the infant began suckling, likely due to the pain associated with breast engorgement. As nursing progressed, the breast seemed to soften, likely relieving the pain.
At 11:30 h on Day 3, the father was holding the infant again, impeding the infant's access to the mother for breastfeeding. At this time, the infant's weight had decreased to 23 g, requiring further intervention as follows. The father was separated from the family, and the infant was syringe-fed 0.8 mL of formula and encouraged to breastfeed. At 13:30 h and 16:30 h, a combination of 0.9 mL of formula and breastfeeding occurred. At 18:30 h, the infant weighed 25g and both mother and child seemed to be well accustomed to the breastfeeding support (Figure 4). Formula supplementation was discontinued at this point to avoid overfeeding. Body weight increased to 26.8 g on Day 4 and 28 g on Day 5. With repeated breast massage and encouragement of the infant's active exploration, the infant quickly learned to breastfeed and showed steady weight gain (Figure 4, postnatal day (PD) 12). In addition, the mother began to facilitate breastfeeding by actively raising her arms (Figure 4D).
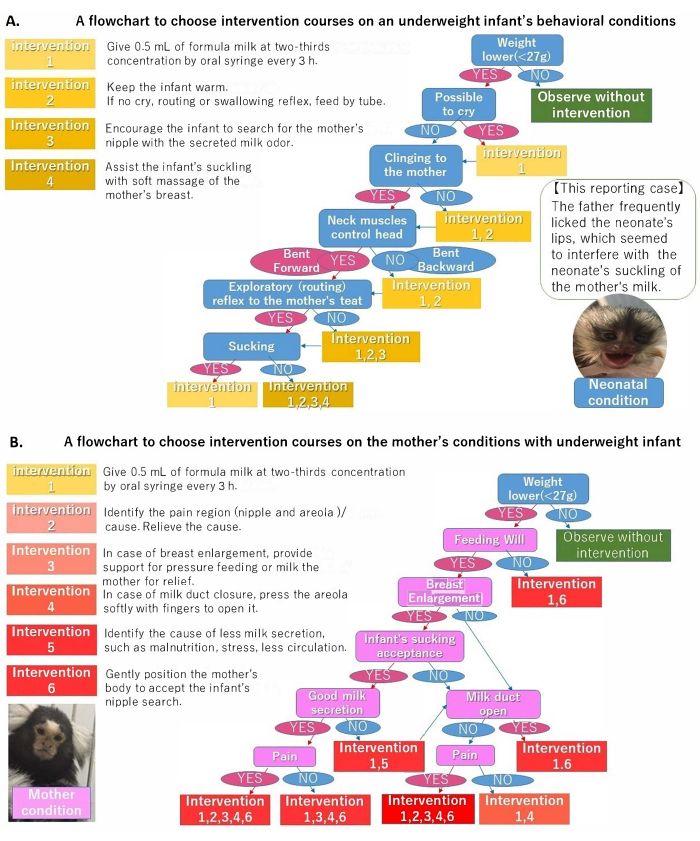
Figure 1: Two diagnostic and intervention flowcharts on common marmoset infant-mother breastfeeding. (A) Infant; (B) mother. Please click here to view a larger version of this figure.
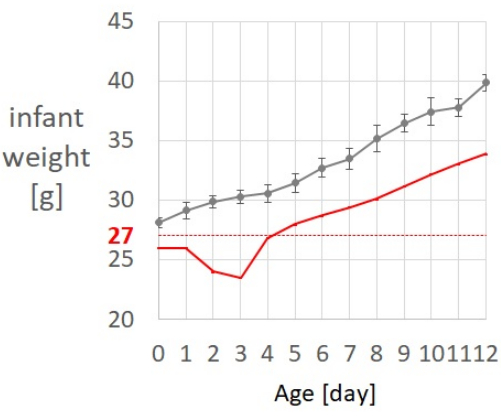
Figure 2: Weight comparison with the averages and standard errors of developmental increase and the minimal record of 27 g for survival in our colony. Dark gray dots and lines: Body weight averages and standard errors in 10 neonatal infants. Red line: This study case of maldevelopment in a neonatal infant. Please click here to view a larger version of this figure.
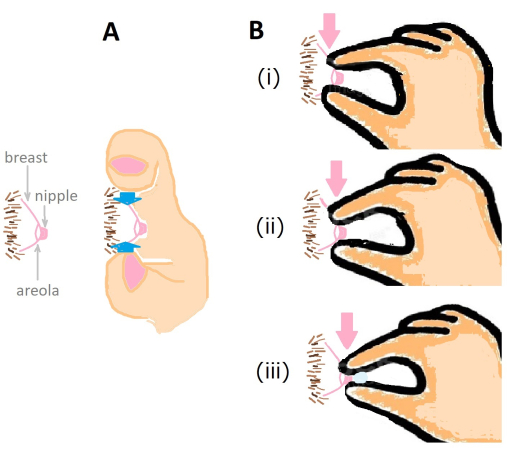
Figure 3: Mother's breast massage to support milk secretion by opening the milk duct and secreting milk. (A) Side pressure (blue arrow) for breast milk secretion. (B) Three steps of fingers' pinch from the base of areolas toward nipples to open the milk ducts.*Note that the hand approaching directions are different between A and B. Please click here to view a larger version of this figure.
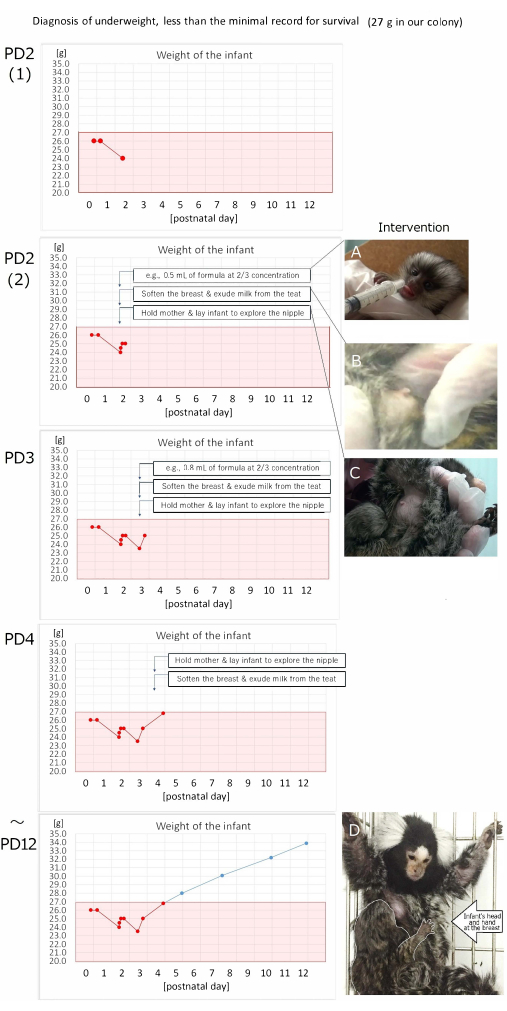
Figure 4: Diagnosis of underweight, less than the minimal record for survival. The infant's weight records from postnatal day (PD) 2 (required intervention for survival) to 12 (the standard increase, approximately 1 g per day) indicate the developmental conditions before and after three types of interventions A, B, and C with the goal behavioral example D. (A) Formula supplementation by syringe. (B) Softening the breast and exuding milk from the teat. (C) Holding the mother and laying the infant to explore the nipple. (D) The mother's cooperative posture during breastfeeding with the infant. Please click here to view a larger version of this figure.
Supplemental Figure S1: Crown, rump, length measurement of the infant marmoset. Please click here to download this File.
