About 330° decompression can be achieved by using the unilateral PVCR technique. The transverse process and the rib head need to be removed to make sure the abduction angle is enough to remove the contralateral bone.
By using the modified trephine, the bone of the diseased vertebrae can be removed easily by rotating it with mild stress. When the trephine is locked, one should pull out the trephine and probe together, and then a cylinder of cancellous bone can be obtained (Figure 2).
Not all patients require a pedicle screw implantation in the osteotomy segment. For some patients with mild vertebral compression and preoperative computed tomography showing there is enough space to implant a pedicle screw, the screw can be implanted on the opposite side of the osteotomy segment. The screw does not need to be taken out once it is implanted because instability can happen without screw fixation. If a patient is eligible for the implantation, it means the patient's segment that needs osteotomy has enough bones. The range of osteotomy can be reduced appropriately on the opposite side as long as it does not interfere with the osteotomy side.
In previous studies, compared to traditional PVCR, unilateral PVCR achieved a satisfactory result but reduced the operating time (174.6 min ± 26.7 min vs. 226.4 min ± 32.6 min), the blood loss (870.3 mL ± 92.5 mL vs. 997.4 mL ± 107.3 mL), and the incidence of nerve root impingement (4.3% vs. 8.7%)13. With the use of the modified trephine, we further shortened the osteotomy time and gained satisfactory treatment results11. In addition, we were able to combine the unilateral PVCR technique and modified trephine to remove the lesions and rebuild spinal stability for patients with Kummell disease (Figure 3 and Figure 4)9,14, especially for patients with kyphotic deformity and obvious nerve-oppressed symptoms.
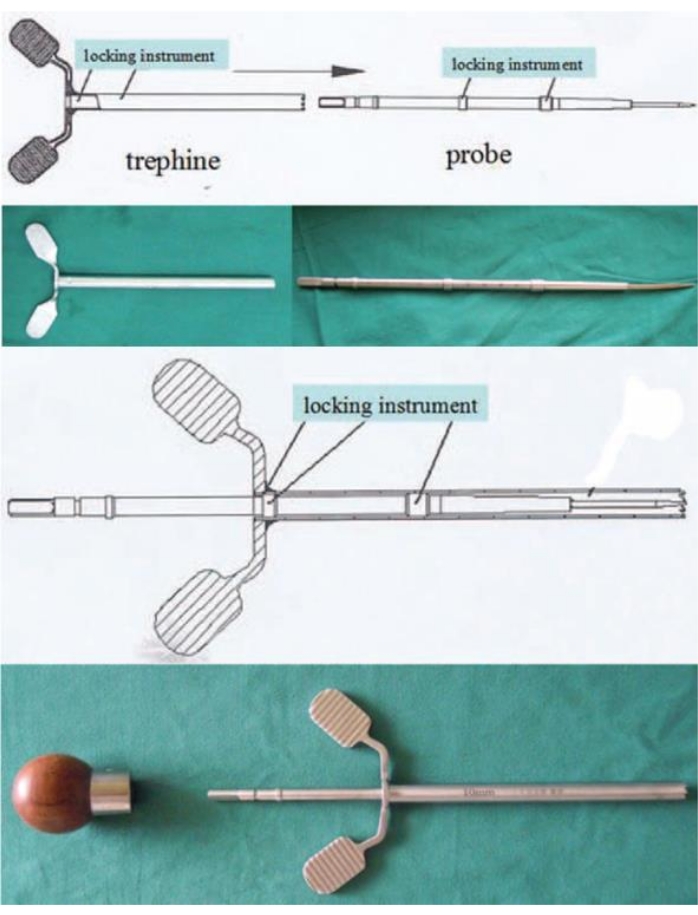
Figure 1: The modified trephine with the locking instrument. Use the probe to stab into the cancellous bone, and then rotate and push the trephine until it is locked. Put on the handle, and then pull out the probe and trephine together. This figure has been modified from Wang et al.11. Please click here to view a larger version of this figure.
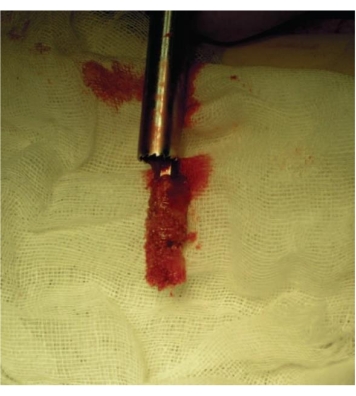
Figure 2: The bone removed by the trephine. Grab the handle of the probe and pull it out, and a columnar bone can be harvested. This figure has been modified from Wang et al.11. Please click here to view a larger version of this figure.
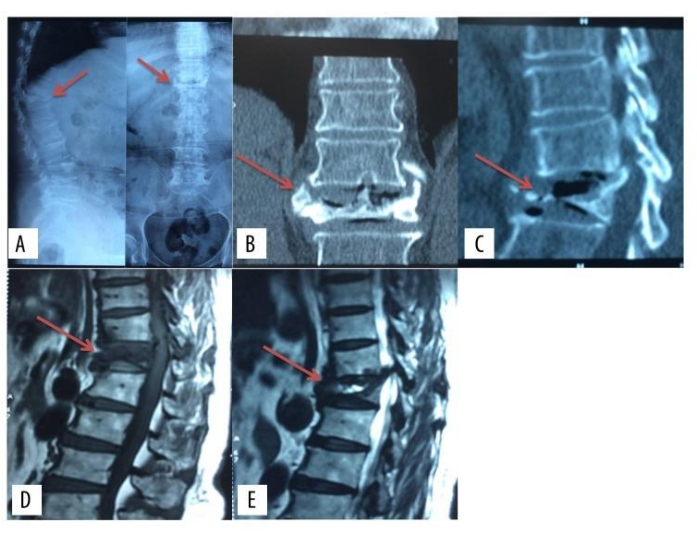
Figure 3: Preoperative images of the unilateral PVCR technique. Preoperative images of X-ray, computed tomography, and magnetic resonance imaging of a patient with Kummell Disease. This figure has been modified from Yang et al.9. Please click here to view a larger version of this figure.
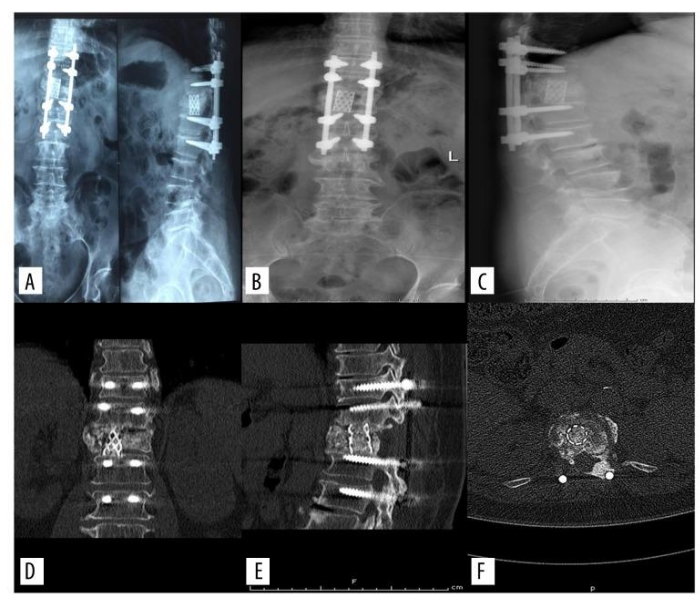
Figure 4: Postoperative images of the unilateral PVCR technique. Postoperative images of X-ray and computed tomography of a patient with Kummell Disease after the treatment of modified posterior vertebral column resection. This figure has been modified from Yang et al.9. Please click here to view a larger version of this figure.
