1. Preparation of a synthetic DNA fragment
- Design and order a synthetic DNA fragment containing the target amplification region for use as a quality control.
- Ensure that the sequence contains the entire amplicon sequence from the forward primer to the reverse primer of the target gene of interest, with an extension of four to six base pairs of sequence at the 5' ends of each primer binding sequence.
- Avoid homopolymers of adenine and thymine greater than 12 base pairs or guanine and cytosine base pairs greater than eight base pairs, as long homopolymers may interfere with synthesis of the gene fragment.
NOTE: If amplicons contain such sequences, base substitutions may be made as long as the annealing sites for the primers and probes are maintained. - Alternatively, prepare a linearized plasmid containing the amplicon using typical cloning strategies.
- Centrifuge the tube containing the synthetic DNA fragment in a microcentrifuge for ~10 s to ensure material is collected at the bottom of the tube.
- Resuspend the synthetic DNA fragment using tris-EDTA (TE) buffer to a concentration of 1.0 × 1010 copies/µL, or as appropriate based on the target assay range.
- Vortex briefly, then incubate at 50 °C for 20 ± 5 min. Cool on ice.
- Prepare multiple, ideally single-use aliquots and store at -70 to -90 °C until use.
NOTE: Synthetic DNA fragments prepared in this manner are typically stable for at least 24 months from the date of resuspension. - If desired, determine the exact concentration of the prepared synthetic DNA stock prior to use as a quality control, or estimate the nominal concentration based on the resuspension utilized.
2. Preparation of primers and probe
- Design and order primers and a hydrolysis probe to target the desired amplification region using typical design strategies26,27.
- Utilize a 5' fluorescent reporter dye (e.g., FAM) and a 3' quencher (e.g., Iowa Black dark quencher) compatible with the ddPCR system.
NOTE: Numerous PCR assay design software packages exist, and any may be utilized. For example, Primer-BLAST by the National Center for Biotechnology Information28 is widely used due to the robust options for assay design and the ease at which specificity can be bioinformatically assessed to identify possible off target effects. It should be noted that the preparation of primers and probes may vary from the steps listed here depending on the format in which they are supplied.
- Utilize a 5' fluorescent reporter dye (e.g., FAM) and a 3' quencher (e.g., Iowa Black dark quencher) compatible with the ddPCR system.
- Centrifuge the tubes containing the forward primer, reverse primer, and probe in a microcentrifuge for ~10 s to pellet material to bottom of the tube.
- Resuspend the primers to 20 µM using TE buffer. Vortex briefly.
- Resuspend the probe to 10 µM using TE buffer. Vortex briefly.
- Prepare multiple, ideally single-use aliquots and store at a minimum of -20 °C until use.
NOTE: Primers and probes prepared in this manner are typically stable for at least 24 months from the date of resuspension.
3. Preparation of sample dilution buffer
- Thaw PCR buffer and sheared salmon sperm DNA at room temperature. Vortex thoroughly to mix.
- Prepare a sample dilution buffer, as per Table 1.
- Vortex thoroughly. Store at 2-8 °C for up to 1 month following preparation.
Table 1: Preparation of sample dilution buffer. Please click here to download this Table.
4. Preparation of master mix
- Thaw the ddPCR master mix for probes, forward primer, reverse primer, and probe at room temperature and allow to warm for at least 10 min post-thaw prior to use. Store at room temperature until use.
NOTE: These reagents must be fully brought to room temperature to ensure efficient droplet formation. Do not hold reagents on ice during preparation.- Vortex thoroughly and briefly centrifuge in a mini centrifuge prior to use.
NOTE: Restriction enzymes are typically supplied in glycerol and should be removed from storage immediately prior to use. Mix gently. Do not vortex.
- Vortex thoroughly and briefly centrifuge in a mini centrifuge prior to use.
- Prepare a PCR master mix for each amplification target. See Table 2 for a suggested PCR master mix composition and modify the concentrations of primers and probes as required.
- Thoroughly vortex and briefly centrifuge prior to the addition of restriction enzyme. Add the restriction enzyme and invert to mix.
NOTE: In this step, 22 µL of PCR reaction is required to obtain a final volume of 40 µL of PCR reaction after droplet formation (consisting of 15 µL of PCR master mix, 5.0 µL of template, and 20 µL of droplet generation oil).
- Thoroughly vortex and briefly centrifuge prior to the addition of restriction enzyme. Add the restriction enzyme and invert to mix.
- Add 16.5 µL of master mix to each well according to the plate map. See Figure 1 for an example plate map for a validation accuracy and precision run.
- Ensure that a plate contains three independent preparations of the quality control (QC) series, three independently tested endogenous tear aliquots tested, spiked to a high and low level and unspiked, and three independent no template controls (NTCs).
- Vary the layout of these wells across the plate, where Set 1 is loaded in order of decreasing concentration, Set 2 is loaded in order of increasing concentration, and Set 3 is loaded in a random order to evaluate if there are any plate location-specific effects.
- Array the samples to fill as much of a column as possible and fill unused wells within a column with control buffer. Include multiple endogenous control lots (e.g., more pools of tears or tears collected from individuals) in the remaining wells, if desired.
- Seal the plate with clear adhesive film. Hold the plate at room temperature during template preparation. Alternatively, hold the plate for up to 4 h at 2-8 °C, but bring it back to room temperature for at least 10 min prior to template addition.
Table 2: Example PCR master mix preparation. Please click here to download this Table.
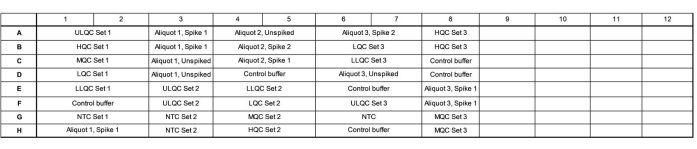
Figure 1: Example plate map for validation accuracy and precision run. Abbreviations: ULQC = upper limit quality control; HQC = high quality control; MQC = medium quality control; LQC = low quality control; LLQC = lower limit quality control; NTC = no template control. Please click here to view a larger version of this figure.
5. Preparing QCs
- Thaw synthetic DNA fragments or linearized plasmids at room temperature and allow to warm for at least 10 min post-thaw prior to use. Bring the templates to room temperature to ensure efficient droplet formation.
- Store at room temperature until use. Vortex thoroughly and briefly centrifuge in a mini centrifuge prior to use.
- Prepare QC dilutions utilizing the sample dilution buffer as the diluent. An example of the recommended concentrations to prepare for a validation accuracy and precision run is presented in Table 3.
NOTE: Following the successful completion of accuracy and precision runs, only the high quality control (HQC), medium quality control (MQC), and low quality control (LQC) need be run on each plate. For accuracy and precision runs, at least three independent dilutions of the QCs are included for the assessment of intra-assay accuracy and precision. Following accuracy and precision runs, only one dilution series need be included. - Following preparation, store the dilutions at room temperature until added to the plate.
- Store the dilutions on ice or at 2-8 °C if needed. Prior to subsequent use, allow the dilutions to warm to room temperature for at least 10 min prior to use. Discard the QCs at the end of the day.
Table 3: Example quality control (QC) preparation using synthetic double-stranded DNA fragments. Abbreviations: ULQC = upper limit quality control; HQC = high quality control; MQC = medium quality control; LQC = low quality control; LLQC = lower limit quality control; NTC = no template control. Please click here to download this Table.
6. Preparation of samples
- Thaw tear samples collected from a clinical trial at room temperature until thawed and allow to warm for at least 10 min post-thaw prior to use.
- Store at room temperature until use. Vortex thoroughly and briefly centrifuge in a micro centrifuge prior to use.
- Dilute tear samples 1:10 (or greater) using sample dilution buffer as the diluent into 0.2 mL PCR tubes or 8-well PCR strips. Seal the tubes.
NOTE: Depending on the expected concentration of target in tears, it may be necessary to further dilute the samples or to test multiple dilutions of each sample. - Heat the samples in a thermal cycler at 95 °C for 10 min, followed by holding at 4 °C for at least 5 min to cool. Use a ramp rate of 3 °C/s.
NOTE: Samples may stay in the thermal cycler at 4 °C until use on the same day or may be frozen at -70 to -90 °C for longer storage. This step serves to denature the vector capsid, releasing the genome. As QC synthetic DNA fragments or linearized plasmids are double stranded, they should not undergo this heating step. - Return the samples following cooling to room temperature (or if frozen, thaw at room temperature) and allow to warm for at least 10 min.
NOTE: The samples must be fully brought to room temperature to ensure efficient droplet formation.
7. Template addition
- Retrieve the ddPCR plate containing the master mix. Vortex each sample or QC dilution tube thoroughly and briefly centrifuge to recollect the material.
- Remove adhesive film and add 5.5 µL of QCs or samples to appropriate wells of the 96-well plate, as per the plate map.
NOTE: Refer to step 4.2.1 for explanation of the required volumes - Add 5.5 µL of sample dilution buffer to the NTC wells.
- Droplet generation requires that all wells of a column have a reaction or buffer control. If any wells of a column do not contain sample reactions, dilute 2x ddPCR buffer control 1:2 using nuclease free water. Add 22 µL of 1x ddPCR buffer control to any empty wells of a column.
NOTE: If an entire column is not used, it is not necessary to add buffer control to these wells. - Add a pierceable foil seal to the plate. Place the plate in the plate sealer and seal for 5 s at 180 °C.
- Alternatively, seal the plate in accordance with the ddPCR system manufacturer's recommendations.
- Vortex the plate at maximum speed for at least 30 s (using the continuous vortexing setting; do not use touch vortexing) and centrifuge briefly in a plate spinner.
NOTE: Thorough and complete mixing of the plate at this step is critical for proper partitioning of the PCR reaction into droplets. Ensure that there are no bubbles visible in the wells. If necessary, the plate can be held at 2-8 °C prior to droplet generation for a maximum of 4 h. If held, allow the plate to come to room temperature for a minimum of 10 min prior to droplet generation.
8. Automated droplet generation, thermal cycling, and droplet reading
- Generate droplets in the automated droplet generator as follows.
- On the touch screen, select the columns on the plate map containing samples. The deck of the instrument will light up to indicate which consumables (DG32 cartridges, tips, waste container, droplet generation oil) are required. Yellow lights indicate that it is necessary to add a consumable, while green lights indicate sufficient consumables are available.
- Load the droplet generator from back to front.
- For hydrolysis probes, ensure that the droplet generation oil for probes is installed and sufficient oil for the number of wells remains. If alternative PCR chemistries are utilized, ensure that a compatible droplet generation oil is installed.
- Place a cold block in the droplet plate holder. Ensure that the block is fully blue colored and no pink is visible. Place a new 96-well ddPCR plate in the cold block.
- Place the prepared PCR plate in the sample plate holder. Close the machine lid. Press start for droplet generation.
- Following droplet formation, a total of 40 µL per reaction is transferred automatically to the new PCR plate.
- Within 30 min following the completion of droplet generation, remove the plate containing the droplets from the cold block. Work gently as the droplets are most fragile at this stage.
- Add a pierceable foil seal to the plate. Place the plate in the plate sealer and seal for 5 s at 180 °C.
- Alternatively, seal the plate in accordance with the ddPCR system manufacturer's recommendations.
- Place the plate in a compatible thermal cycler. Enter the cycling conditions (see Table 4).
- Following the end of thermal cycling, hold the plate in the thermal cycler, transferred to 2-8 °C, or read it immediately.
NOTE: Holding the plate for 12 h at 4-12 °C may improve droplet counts, but this is not required. Sufficient droplets should be obtained without the hold. - Load the plate into the droplet reader, ensuring sufficient reader oil remains and the waste container has sufficient space. Read the droplets. Perform droplet reading within 24 h of thermal cycling initiation.
Table 4: Typical thermal cycling conditions. Please click here to download this Table.
9. Data analysis
NOTE: A minimum of 10,000 droplets per well is necessary for the proper calculation of concentration using Poisson statistics. Do not attempt analysis on any wells with fewer than 10,000 droplets.
- A threshold is required to define the droplets as positive or negative. The ddPCR analysis software automatically applies a threshold that may vary across wells. However, manually set a threshold for all wells of the plate at slightly above the fluorescent intensity of the NTC wells for more consistent, accurate, and precise results.
NOTE: Proper placement of the threshold may require optimization depending on the separation of the positive and negative droplets and how much droplet rain exists (see Figure 2). In this example, the droplet amplitude graph shows example wells at each QC level and the NTC. The purple line indicates a threshold of 1,000, set slightly above the negative droplet population. - Poisson statistical modeling requires at least three positive droplets to calculate the concentration with 95% confidence. Consider all wells containing zero, one, or two positive droplets to be negative and set to a concentration of zero27.
- Back-calculate the copy number in each tear sample.
- The concentration, in copies/µL, is provided in the data report. Use this value to determine the concentration in copies/µL of the original sample (i.e., in the tear sample).
- To calculate the ddPCR reaction dilution, divide the initial PCR reaction volume prior to droplet formation by the volume of template added. When the volumes presented in this method are utilized, this yields a value of 4.
- Determine the serial dilution factor from the original sample (step 6.2).
- To determine the copies/µL in the sample, multiply the copies/µL by the ddPCR reaction dilution, then by the serial dilution factor. For example, the concentration in copies/µL generated in the data report was 966; 5.5 µL of template was added per 22 µL of reaction. A 1:50,000 serial dilution of the sample was utilized.


- If multiple dilutions of the same sample were tested, analyze all valid, in-range dilutions and calculate the mean.
- For each QC, calculate the expected copies/µL PCR reaction by dividing the concentration of the given QC dilution (in copies/µL) by the ddPCR reaction volume (20 µL). This allows for direct comparison of this nominal value to the copies/µL value provided in the data report without further calculations.
NOTE: This approach was also used for analysis of the spiked tear samples utilized in the representative results. - Determine the mean value, standard deviation, coefficient of variation (%CV), and percent relative error to the nominal concentration (%RE) of the sample or QC value using the replicate wells (include multiple dilutions if applicable).
- For the assessment of inter-well precision, determine this for each of the well duplicates, if included.
- For the assessment of intra-assay accuracy and precision, determine this for each dilution series or aliquot utilized within a batch.
- For the assessment of inter-assay accuracy and precision, determine this using the intra-assay means of each of the included batches.
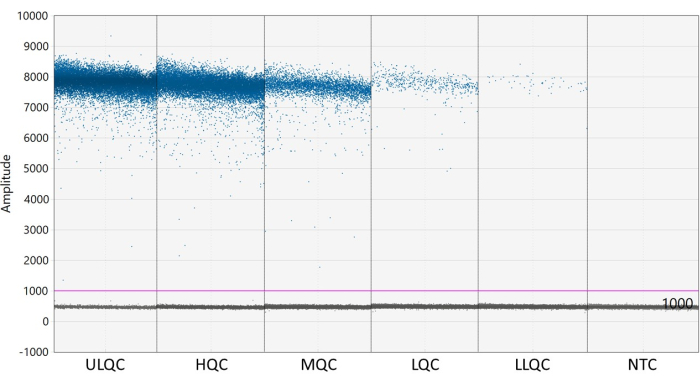
Figure 2: Example of setting threshold. Abbreviations: ULQC = upper limit quality control; HQC = high quality control; MQC = medium quality control; LQC = low quality control; LLQC = lower limit quality control; NTC = no template control. Please click here to view a larger version of this figure.
10. Assay acceptance criteria
- Utilize the following specifications to the calculated data for each batch to determine if the batch is acceptable. If these conditions are not met, invalidate and repeat the batch.
NOTE: These criteria were determined as a consensus from published white papers on PCR-based assay validation18,19,20,21,22,23,24,25. It may be necessary to modify the target criteria as appropriate for clinical application. - No template control (NTC)
- Ensure that each NTC well has at least 10,000 droplets.
- Ensure that each NTC well has less than 3 positive droplets.
- QCs and assay range
- Ensure that each QC well has at least 10,000 droplets.
- Make sure that the precision of replicate wells of a QC concentration is ≤25.0% CV, except at the upper and lower limits of quantification, where ≤30.0% is acceptable. Assess this independently for each QC set and concentration level.
- Ensure that the relative error of the back-calculated concentration at each mean QC level is within ±25.0% RE of the nominal concentration (copies/PCR reaction), except at the upper and lower limits of quantification, where ±30.0% RE is acceptable. Assess this independently for each QC set and concentration level.
- Make sure that at least 2/3 of the QC samples (e.g., four out of six results) and 50% of the QC samples at each level (low, medium, high) meet these guidelines.
- Samples
- Ensure that the sample wells to be analyzed have at least 10,000 droplets.
- Make sure that the precision of replicate wells of a sample dilution to be analyzed is ≤25.0% CV.
- Ensure that at least one included dilution of the given sample is within the defined quantification range of the assay, as defined above based on the upper and lower limit QCs.
- If all dilutions included yield results greater than the defined upper limit of quantification, and if a sufficient sample volume remains, repeat the assay using a higher dilution of the sample.
- If all dilutions included yield a result lower than the lower limit of quantification, and if a sufficient sample volume remains, repeat the assay using a lower dilution of the sample.
NOTE: Samples containing more than three positive droplets, but that have a concentration below the lower limit of quantification, can be described as detectable, but not quantifiable.
