The above-mentioned structured approach to an EBUS-TBNA procedure has been taught at CAMES since 2016 as part of the EBUS-certified training program offered by the European Respiratory Society (ERS)7. The 6 landmarks approach is based on a validated assessment tool for measuring competency in EBUS-guided transbronchial needle aspiration4. By performing EBUS-TBNA in a structured way, as shown above, no important lymph nodes will be missed, and the diagnostic accuracy will be very high.
As described in the protocol and shown in the video, we suggest a very structured approach to the EBUS procedure to make sure no essential lymph nodes will be missed.
It is important to note that the order mentioned above (station 4L (Figure 4)→ station 7 (Figure 5) → station 10L/11L (Figure 6) → station 10R/11R (Figure 7) → azygos vein (Figure 8) → station 4R (Figure 9)) is the initial diagnostic approach to ensure that the procedure is done systematically (Figure 10).
However, if radiology has shown a suspicious mass or lymph node on the left side, it will be correct to start on the right side as far away from the tumor as possible.
Several studies have shown that a systematic approach is important when performing endoscopic pulmonary procedures (Table 1)11,12,13. Sanz-Santos et al. compared systematic and targeted staging in 107 patients and found that systematic EBUS-TBNA sampling provided additional important clinical information in 14 cases (13%) compared to targeted EBUS-TBNA12. Similar results were found by Crombag et al. in 2019, showing that systematic EBUS was superior to PET-CT-targeted EBUS alone13.

Figure 1: EVIS Exera II endoscopy tower with a BF-UC180F EBUS endoscope (Olympus, Japan). Please click here to view a larger version of this figure.
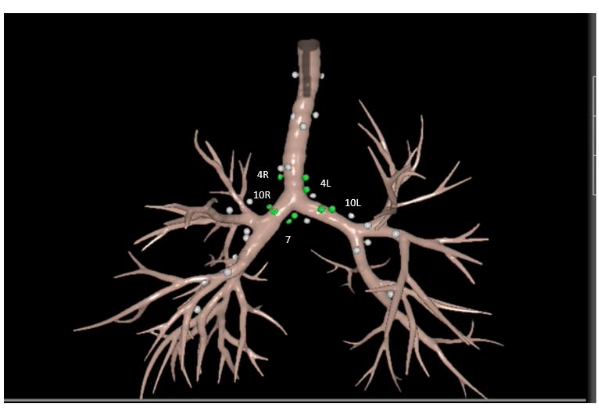
Figure 2: Location of the mediastinal lymph nodes. Stations 4R, 4L, 7, 10R and 10L are highlighted. Picture from Surgical Science Simulator, GI-Bronch Mentor, Essential Bronchoscopy Task 4. Lung Anatomy, Lymph Nodes. Please click here to view a larger version of this figure.
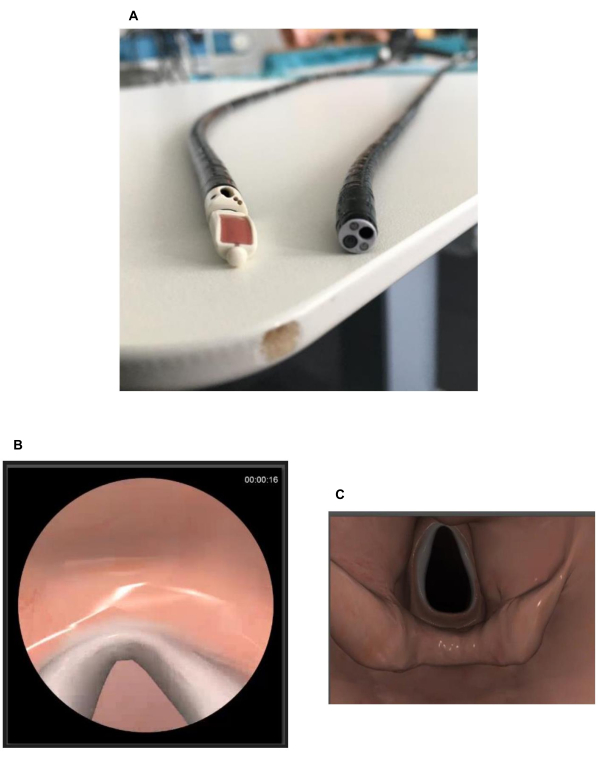
Figure 3: Differences between the endoscope and the bronchoscope. (A) The end of the endoscope compared to the end of a bronchoscope showing the endoscope's oblique angle view as the ultrasound transducer reduces the visibility.(B) The vocal cords seen from the endoscope. (C) The vocal cords from a bronchoscope. Please click here to view a larger version of this figure.
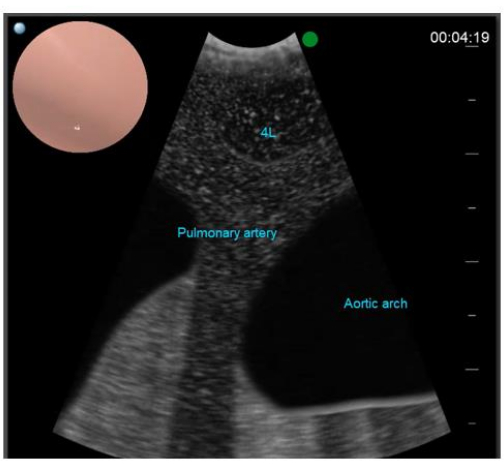
Figure 4: Landmark 1. Station 4L is located at the left side of the trachea, just cranial to the carina. Picture from Surgical Science Simulator, GI-Bronch Mentor, Essential EBUS Case 6. Please click here to view a larger version of this figure.
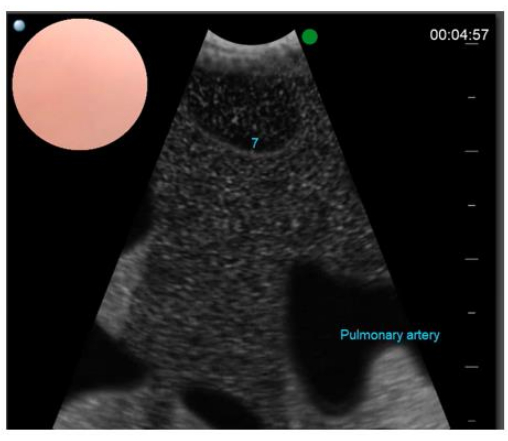
Figure 5: Landmark 2. Station 7 is found between the right pulmonary artery and the left atrium below the carina. Picture from Surgical Science Simulator, GI-Bronch Mentor, Essential EBUS Case 6. Please click here to view a larger version of this figure.
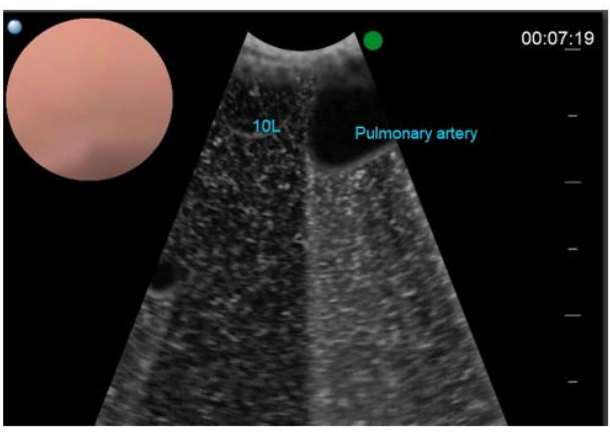
Figure 6: Landmark 3. Station 10L is located adjacent to the left main bronchus cranial to the left upper lobe. Picture from Surgical Science Simulator, GI-Bronch Mentor, Essential EBUS Case 6. Please click here to view a larger version of this figure.
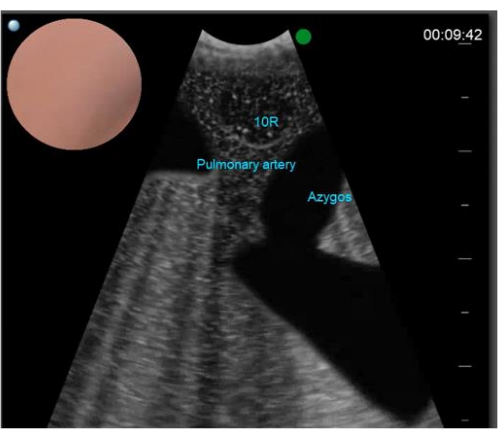
Figure 7: Landmark 4. Station 10R is located on the right side of the right main bronchus, just caudal to the inferior border of the azygos vein. Picture from Surgical Science Simulator, GI-Bronch Mentor, Essential EBUS Case 6. Please click here to view a larger version of this figure.
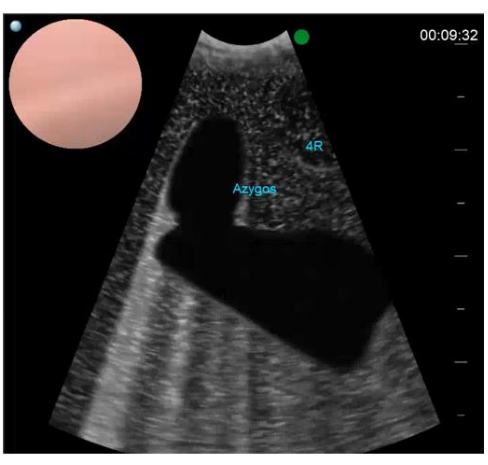
Figure 8: Landmark 5. The azygos vein can be found by turning the transducer clockwise in the trachea. The figure shows how the azygos vein drains into the superior vena cava. Picture from Surgical Science Simulator, GI-Bronch Mentor, Essential EBUS Case 6. Please click here to view a larger version of this figure.
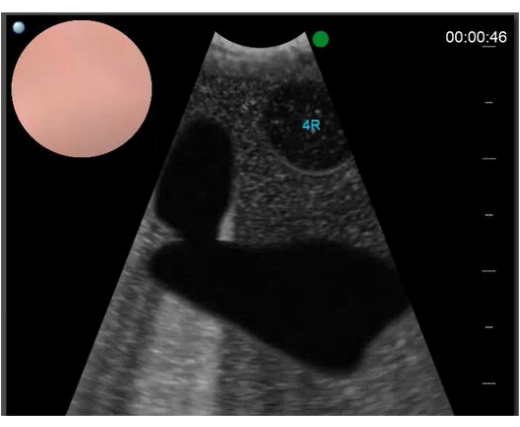
Figure 9: Landmark 6. Station 4R is found to the right or anterior to the trachea above the lower border of the azygos vein. Picture from Surgical Science Simulator, GI-Bronch Mentor, Essential EBUS Case 6. Please click here to view a larger version of this figure.
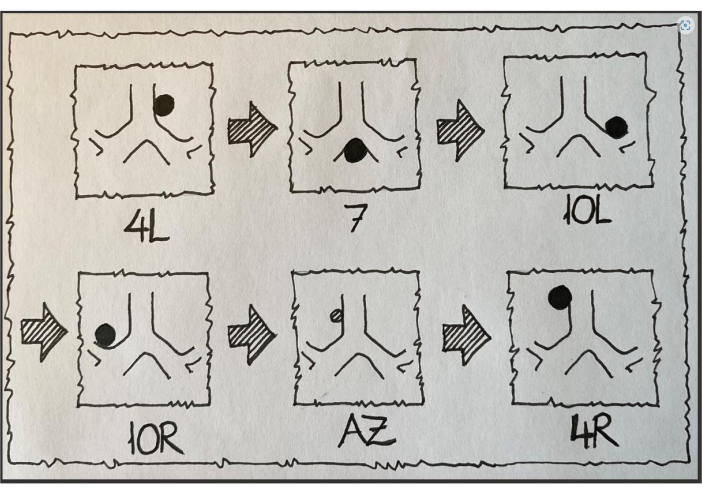
Figure 10: Overview of the six EBUS landmarks. AZ, azygos vein. Illustration by Paul Frost Clementsen, 2023. Please click here to view a larger version of this figure.
| Targeted EBUS by PET-CT | Systematic EBUS-TBNA | Reference | ||||||
| 107 patients staged with N2 disease | Provided additional clinical information in 14 (13%) of the 107 patients (3 patients upstaged with N3 disease + 11 patients with N2b disease [staged as N2a disease on PET-CT]) | 12 | ||||||
| Sensitivity 73% (75/103) Negative predictive value 81% (122/150) | Sensitivity 77% (79/103) Negative predictive value 84% (122/146) | 13 | ||||||
Table 1: Data comparing targeted EBUS by PET-CT and systemic EBUS-TBNA approaches.
