A schematic diagram of the workflow to detect and quantify HBV DNA from human plasma/serum is shown in Figure 1. An amplification plot of Standard 2 (used as a PC) and NTC for both HBV and IC is shown in Figure 2. Figure 3 shows the amplification curves for an HBV-positive sample, an HBV-negative sample, and a sample with PCR inhibition. The amplification curve, Ct value for HBV, and obtained HBV concentration in international units per microliter (IU/µL) for the NIBSC code 10/266 are shown in Figure 4. Amplification curves for the HBV target of all the 5 HBV standards of the kit and a representative standard curve for the same are shown in Figure 5. The slope of the standard curve is -3.361, R2 is 0.99996, and efficiency is 0.98. Amplification curves for the IC target of all 5 HBV standards are shown in Figure 6.
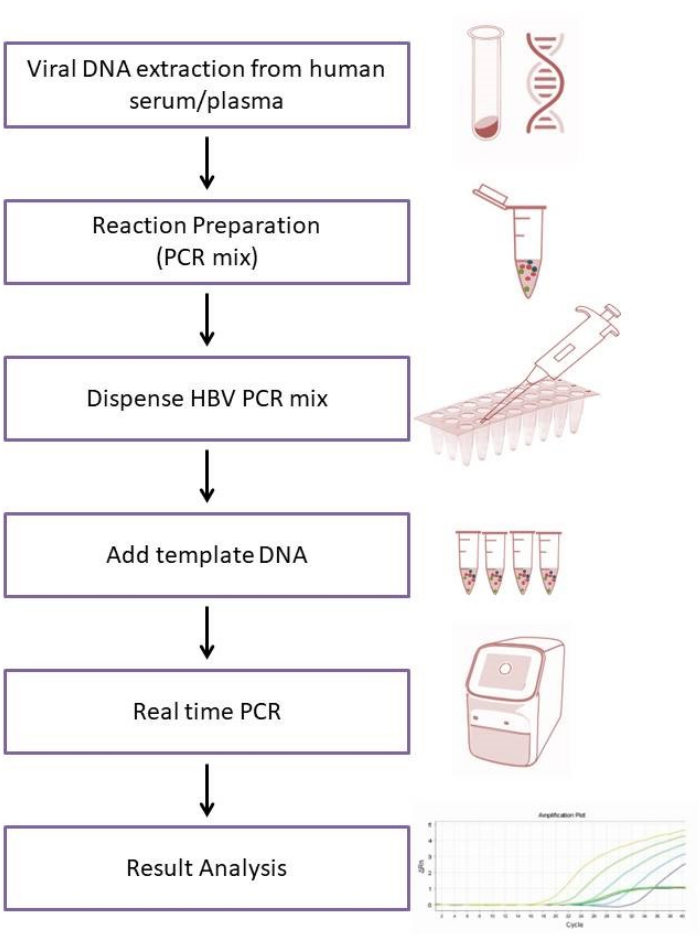
Figure 1: Schematic diagram of the workflow to detect and quantify HBV DNA from human plasma/serum samples. Extract viral DNA from human serum/plasma sample of HBV suspected individual. Prepare the PCR mix by adding each PCR component except the template DNA/ standard(s). Dispense it into PCR tubes/wells. Add the extracted viral DNA/ standard(s) as the template DNA, and close the PCR tubes. Load it into a real-time PCR machine, start the PCR run, and analyze the result after run completion. Please click here to view a larger version of this figure.
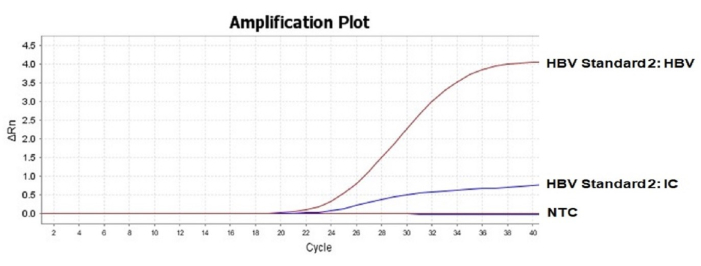
Figure 2: Amplification plot of Standard 2 (used as a PC) and NTC. An amplification plot of HBV standard 2 is shown here for both the HBV and IC targets. For qualitative result analysis, Standard 2 can be used as a positive control. For NTC, no amplification was observed for either of the targets. Please click here to view a larger version of this figure.
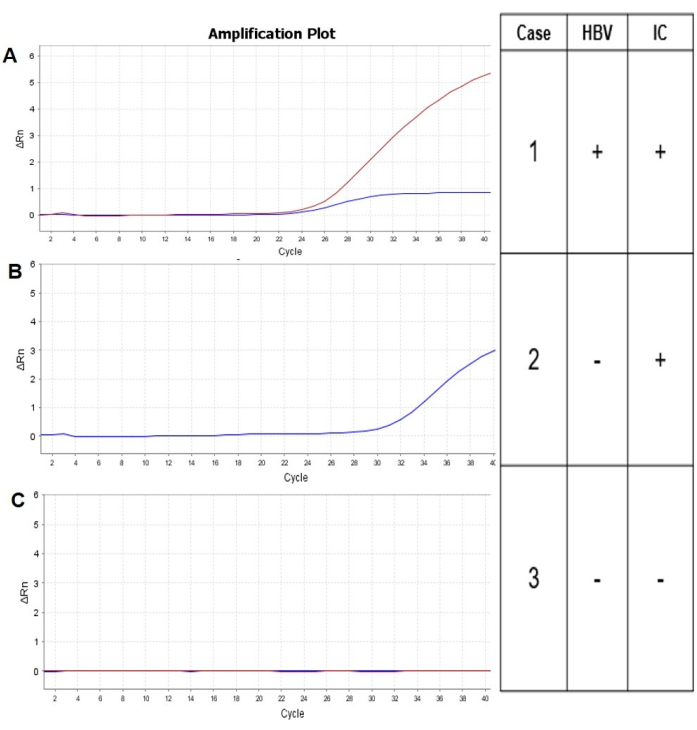
Figure 3: Amplification plots for HBV positive sample, HBV negative sample, and a sample with PCR inhibition. Amplification plots for three different samples: HBV positive (Case 1), HBV negative (Case 2), and a sample containing PCR inhibitors (Case 3) are shown here. In the case of the HBV positive sample, both the targets are amplified, whereas only IC was amplified for the HBV negative sample, and no amplification for the HBV target was observed as expected. Neither HBV nor IC was amplified for Case 3, which means PCR inhibition occurred due to the PCR inhibitors present in the DNA sample used as the PCR template. Please click here to view a larger version of this figure.
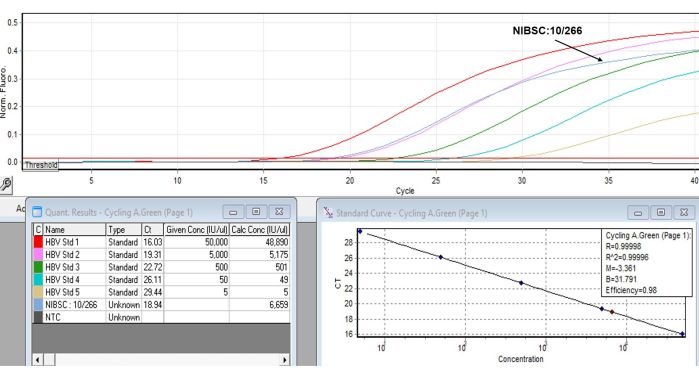
Figure 4: Amplification curve, Ct value for HBV, and obtained HBV concentration (IU/µL) for the NIBSC code 10/266. Extracted viral DNA of NIBSC code 10/266 was run along with the 5 HBV standards and NTC. The amplification curve for the HBV target is shown for the NIBSC code 10/266 sample in the upper panel. Its Ct value for HBV is 18.94, and the calculated concentration is 6659 IU/µL, shown in the lower panel. Please click here to view a larger version of this figure.
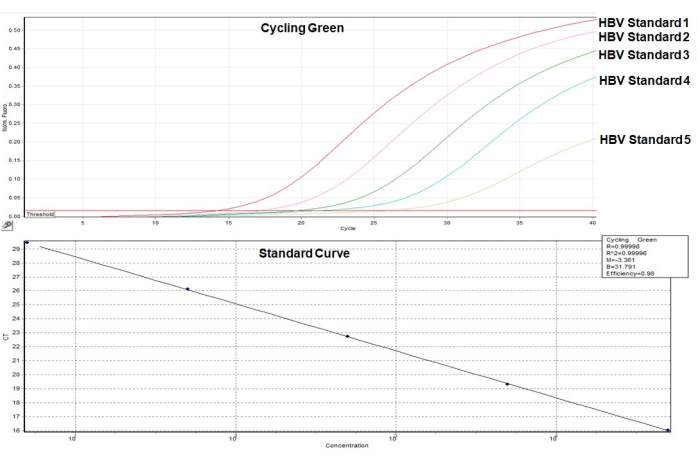
Figure 5: Amplification curves for the HBV target of all 5 HBV standards and the standard curve. Amplification curves for the HBV target (green channel) of all 5 HBV standards are shown in the upper panel. A standard curve along with its slope (3.361), R2 value (0.99996), and PCR efficiency (0.98) are shown in the lower panel. Please click here to view a larger version of this figure.
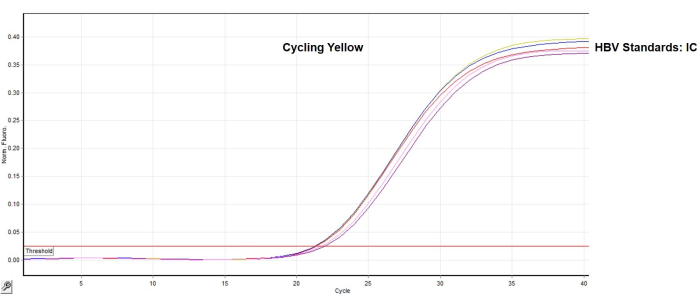
Figure 6: Amplification curves for the IC target of all 5 HBV standards. Amplification curves of 5 HBV standards for the IC (yellow channel) are shown here. As expected, they look the same with similar Ct values. Please click here to view a larger version of this figure.
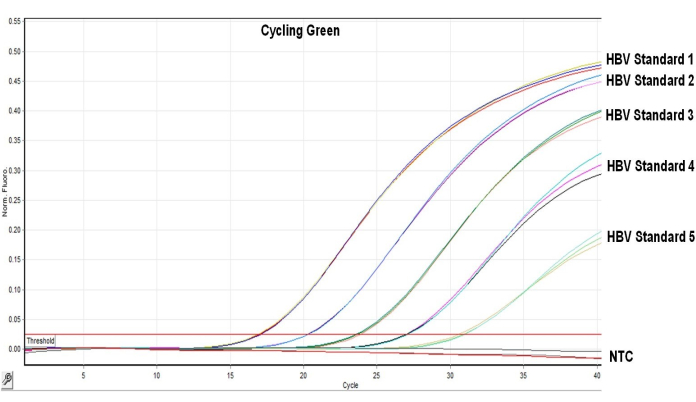
Figure 7: Amplification curves for the HBV target of all 5 HBV standards and NTC were run in triplicate. The amplification plots of three replicates for the HBV target (Green channel) of the 5 HBV standards show similar results. Please click here to view a larger version of this figure.
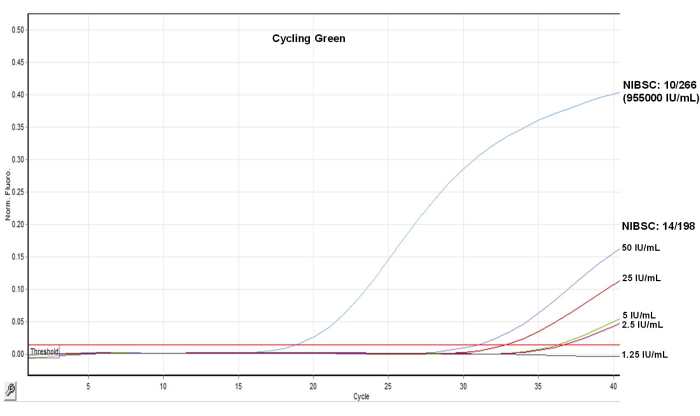
Figure 8: Amplification curves for the HBV target of NIBSC code 10/266, NIBSC code 14/198, and its five dilutions. The amplification curves for the HBV target (green channel) of the reference samples NIBSC code 10/266, NIBSC code 14/198, and its five dilutions (1.25 IU/mL, 2.5 IU/mL, 5 IU/mL, 25 IU/mL, and 50 IU/mL) are shown here. No amplification was detected for 1.25 IU/mL, while other dilutions showed proper amplification curves before 38 Ct. Please click here to view a larger version of this figure.
| Reagent | Description |
| Multiplex master mix | PCR buffer, Hot Start Taq DNA polymerase, and other PCR components |
| HBV primer probe mix | Primers and probe mix for HBV detection |
| Endogenous IC primer probe mix | Primers and probe mix for endogenous internal control (IC) detection |
| Standards for HBV | · HBV Standard 1 |
| · HBV Standard 2 | |
| · HBV Standard 3 | |
| · HBV Standard 4 | |
| · HBV Standard 5 | |
| Negative Control | PCR grade nuclease-free water |
Table 1: Reagents supplied with the real-time PCR kit and their description
| Reagent | Volume per reaction |
| Multiplex master mix | 11 µL |
| HBV primer probe mix | 2 µL |
| Endogenous IC primer probe mix | 2 µL |
| Total reaction volume | 15 µL |
Table 2: Volume of each reagent to be added per reaction for PCR mix preparation
| Step | Temperature (°С) | Time | Data collection | Cycles |
| Initial Denaturation | 94 | 10 min | – | 1 |
| PCR cycling | 94 | 15 s | – | 40 |
| 55 | 60 s | On | ||
| 72 | 15 s | – |
Table 3: PCR cycling conditions
| Target | Rotor-Gene Q* | CFX 96 | ABI real-time PCR# |
| HBV | Green | FAM | FAM |
| IC | Yellow | HEX | VIC |
| *Auto-Gain Optimisation Setup- select 'Perform Optimisation Before 1st Acquisition’ | |||
| #Only for Applied Biosystems’ real-time PCR machines, select ROX as the ‘Passive Reference’ dye during plate setup, as the master mix of the kit contains ROX | |||
Table 4: Dye selection for different real-time PCR platforms
| Real Time PCR Instrument | Dyes | Threshold value range§ |
| ABI real-time PCR¶ | FAM | 0.2–0.25 |
| VIC | 0.05–0.12 | |
| Bio-Rad CFX-96† | FAM | 100–800 |
| HEX | 50–400 | |
| Rotor-Gene Q | Green | 0.015–0.03 |
| Yellow | 0.01–0.02 | |
| §An absolute threshold value varies from instrument to instrument depending upon instrument’s age, model and calibration status | ||
| ¶These threshold values are applicable when ROX is selected as the ‘Passive Reference’ dye | ||
| †Relative fluorescence is increased by about 2 to 5-fold when Bio-Rad's white PCR tubes are used instead of clear tubes. So, the threshold value should be determined accordingly | ||
Table 5: Recommended threshold values for different real-time PCR platforms
| Sample type | Case | Amplification Signal in | Result Interpretation | |||
| FAM/Green | HEX/VIC/Yellow | |||||
| Control | Standard 2/PC | Yes (20 ± 2) | Yes (24 ± 3) | Standard 2/PC is working properly | ||
| NTC | No | No | NTC is working properly | |||
| Sample | 1 | Yes | Yes / No* | HBV specific DNA detected | ||
| 2 | No | Yes | HBV specific DNA not detected. Sample does not contain detectable amount of HBV specific DNA | |||
| 3 | No | No | Possible inhibition of PCR, dilute the DNA sample (1:10) / re-extract DNA from the original sample and repeat the PCR | |||
| *Detection of the Internal Control is not required when the HBV target is detected. High HBV DNA load in the sample can lead to reduction or absence of Internal Control signal | ||||||
Table 6: Result interpretation of positive, negative, and PCR inhibitors containing poor-quality samples
| Standard | Concentration (IU/µl) | Desired Ct | |
| HBV | IC | ||
| (FAM/ Green) | (HEX/VIC/Yellow) | ||
| HBV Standard 1 | 5 X 104 | 17 ± 2 | 24 ± 3 |
| HBV Standard 2 | 5 X 103 | 20 ± 2 | 24 ± 3 |
| HBV Standard 3 | 5 X 102 | 23 ± 2 | 24 ± 3 |
| HBV Standard 4 | 5 X 101 | 27 ± 2 | 24 ± 3 |
| HBV Standard 5 | 5 X 100 | 31 ± 2 | 24 ± 3 |
Table 7: HBV standards and its concentration of the HBV target and desired Ct values
| Sample | Expected Ct | Obtained Ct for HBV | Average Ct | Standard Deviation | CV % | ||
| Replicate 1 | Replicate 2 | Replicate 3 | |||||
| HBV Standard 1 | 17 ± 2 | 17.01 | 16.89 | 17.07 | 16.99 | 0.09 | 0.54 |
| HBV Standard 2 | 20 ± 2 | 20.29 | 20.32 | 20.34 | 20.32 | 0.03 | 0.12 |
| HBV Standard 3 | 23 ± 2 | 23.61 | 23.88 | 23.73 | 23.74 | 0.14 | 0.57 |
| HBV Standard 4 | 27 ± 2 | 26.95 | 27.03 | 27.12 | 27.03 | 0.09 | 0.31 |
| HBV Standard 5 | 31 ± 2 | 30.58 | 30.91 | 31 | 30.83 | 0.22 | 0.72 |
Table 8: Obtained Ct values, average, standard deviation, and coefficient of variation (CV%) of 5 HBV Standards.
