The male/female ratio was 11/9 for the participants. For all the individuals, the age reached 35.35 ± 6.83 years, educational level was 14.80 ± 3.29 years, Hamilton depression scale-17 (HAMD-17) score was 21.95 ± 2.76 points, SE was 76.71 ± 8.57%. Regarding the cognitive screening tool scores, PDQ-5, SPO, SC, CB, TMT-B, and total scores were 1756.35 ± 395.49, 2046.75 ± 684.45, 852.15 ± 651.81, 845.75 ± 641.15, 911.45 ± 619.13 and 4140.80 ± 1298.14 points, respectively (Table 2).
Figure 5 illustrates two representative participants. A female patient with MDD (Figure 5A), aged 49 years, had a lower THNIC-it score, including SPO score = 0, SC score = 0, CB score = 0, and TMT-B score = 680. She had higher SL (40.5 min), WASO (60.5 min), and lower SE (82.2%). A male patient with MDD (Figure 5B), aged 48 years, had a higher score, including SPO score = 1856, SC score = 1250, CB score = 163, and TMT-B score = 1484. He had higher SL (7.0 min), WASO (5.5 min), and lower SE (88.1%). The total score was significantly correlated with SL (r = −0.0856, p < 0.001), WASO (r = -0.687, p = 0.001), and SE (r = 0.081, p < 0.001).
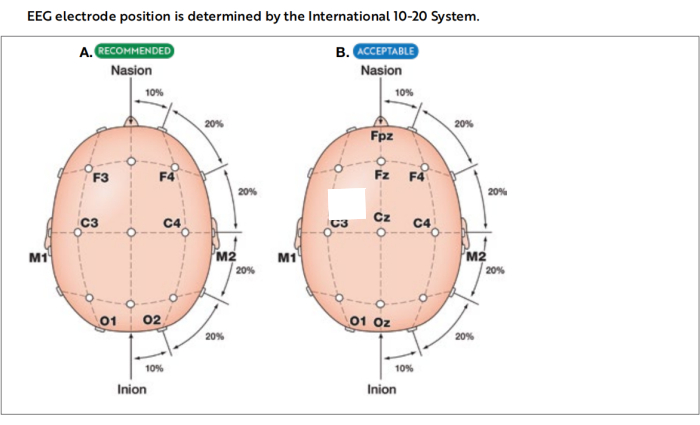
Figure 1: International 10-20 system of electrode placement. Images illustrating the placement of electrodes utilized in recommended (A) and acceptable (B) derivations for electroencephalography (EEG) during polysomnography. This figure has been adapted with permission from The AASM Manual for the Scoring of Sleep and Associated Events18. Please click here to view a larger version of this figure.
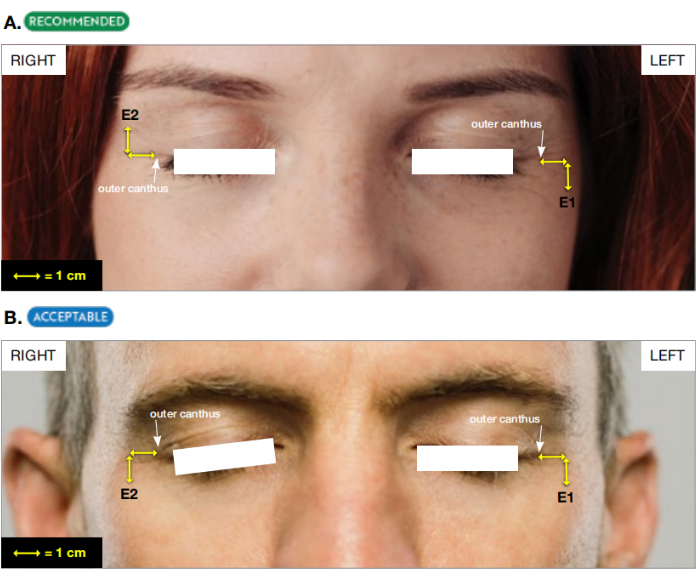
Figure 2: The placement of two derivations of EOG. (A) Recommended and (B) acceptable derivations for electrooculogram (EOG). This figure has been adapted with permission from The AASM Manual for the Scoring of Sleep and Associated Events18. Please click here to view a larger version of this figure.
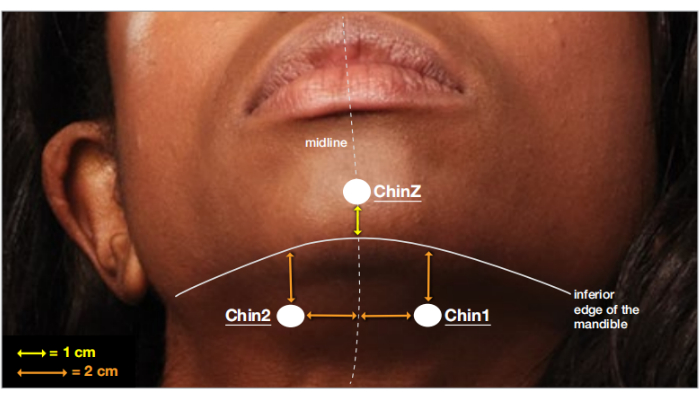
Figure 3: The placement ofthree derivations of chin EMG. Placement of electrodes on the chin for electromyogram (EMG) recording. This figure has been adapted with permission from The AASM Manual for the Scoring of Sleep and Associated Events18. Please click here to view a larger version of this figure.
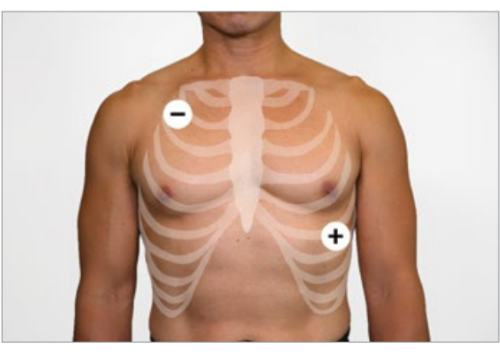
Figure 4: The placement of two derivations of ECG. The diagram shows Lead II placement on the torso during cardiac recording. This figure has been adapted with permission from The AASM Manual for the Scoring of Sleep and Associated Events18. Please click here to view a larger version of this figure.
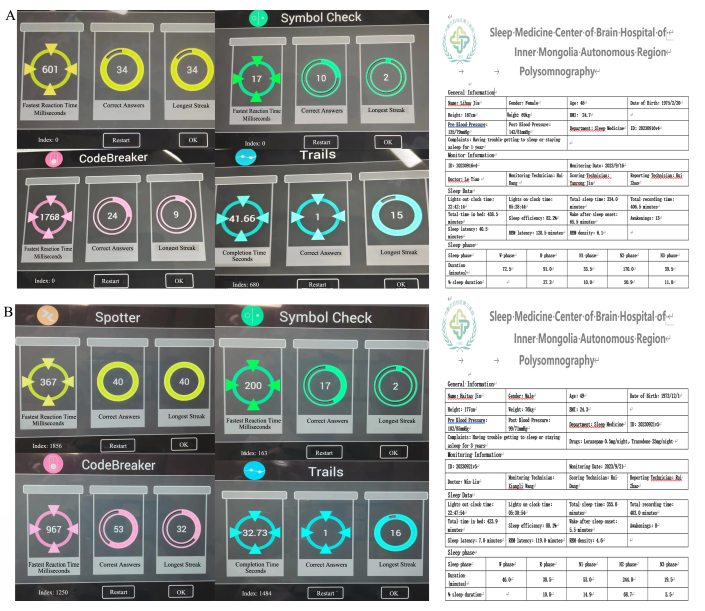
Figure 5. Representative participants. (A) A 49-year-old participant with a lower score also had higher SL (40.5 min), WASO (60.5 min), and lower SE (82.2%). (B) A 49-year-old participant with a higher THNIC-it score also had lower SL (7.0 min), WASO (5.5 min), and higher SE (88.1%). Please click here to view a larger version of this figure.
| Calibration steps to document appropriate system response. |
| 1. Perform and document an impedance check of the EEG and EMG electrodes. |
| 2. Record a minimum of 30 s of EEG with patients awake lying quietly with eyes open. |
| 3. Record a minimum of 30 s of EEG with patients awake lying quietly with eyes closed. |
| 4. Ask the patient to look up and down without moving head (5x). |
| 5. Ask the patient to look left and right without moving head (5x). |
| 6. Ask the patient to blink (5x). |
| 7. Ask the patient to grit teeth and/ or chew (5 s). |
| 8. Ask the patient to simulate a snore or hum (5 s). |
| 9. Ask the patient to breathe normally and assure that an airflow and effort channel signals are synchronized. |
| 10. Ask the patient to perform a breath hold (10 s). |
| 11. Ask the patient to breathe through the nose only (10 s). |
| 12. Ask the patient to breathe through the mouth only (10 s). |
| 13. Ask the patient to flex the left foot /rase toes on left foot (5x). |
| 14. Ask the patient to flex the right foot /rase toes on right foot (5x). |
| 15. Adjust ECG signal to provide a clear waveform-the R wave should deflect upward. |
| 16. Perform and document a repeat impedance check of the EEG, EOG and EMG electrodes at the end of the PSG recording. |
| 17. Repeat impedance measures and physiological calibrations at the end the PSG recording. |
Table 1: PSG calibration procedure. Abbreviations: EEG: Electroencephalogram; EMG: Electromyography; EOG: Electrooculogram; PSG: Polysomnography.
| Gender (male/female) | 11/9 |
| Age (years) | 35.35 ± 6.83 |
| Educational level (years) | 14.80 ± 3.29 |
| HAMD-17 (score) | 21.95 ± 2.76 |
| SE (%) | 76.71 ± 8.57 |
| PDQ-5 (score) | 1756.35 ± 395.49 |
| SPO (score) | 2046.75 ± 684.45 |
| SC (score) | 852.15 ± 651.81 |
| CB (score) | 845.75 ± 641.15 |
| TMT-B (score) | 911.45 ± 619.13 |
| THINC-it total score | 4140.80 ± 1298.14 |
Table 2: Patient demographics and scores. HAMD: Hamilton depression scale; SE: sleep efficiency; PDQ-5: perceived deficits questionnaire; SPO: spotter test; SC: symbol check test; CB: code breaker test; TMT-B: trail making test-B; THINC-it: THINC-integrated tool.
Supplementary Figure 1: Screenshot showing the calibration procedure. Please click here to download this File.
Supplementary Figure 2: Screenshot showing the cognitive screening tool subtests. Please click here to download this File.
