Determination of Cardiac Output in a Porcine Model for Ex Vivo Pulmonary Perfusion
Summary
This protocol describes the surgical technique used for the placement of a thermodilution catheter through the jugular vein in pigs to estimate cardiac output and ensure adequate lung perfusion during ex vivo lung perfusion (EVLP).
Abstract
Due to their physiological similarities to humans, pigs are used as experimental models for ex vivo lung perfusion (EVLP). EVLP is a technique that perfuses lungs that are not suitable for transplantation via an extracorporeal circulation pump to improve their function and increase their viability. Existing EVLP protocols are differentiated by the type of perfusion solution and perfusion flow, which varies from 40%-100% of the estimated cardiac output (CO) according to the body surface area (BSA). Devices for measuring CO use simple physical principles and other mathematical models. Thermodilution in animal models continues to be the reference standard for estimating CO because of its simplicity and ease of reproduction. Therefore, the objective of this study was to reproduce the measurement of CO by thermodilution in pigs and compare its precision and accuracy with those obtained by the BSA, weight, and Fick’s method, to establish perfusion flow during EVLP. In 23 pigs, a thermodilution catheter was placed in the right jugular vein, and the carotid artery on the same side was cannulated. Blood samples were obtained for gasometry, and CO was estimated by thermodilution, adjusted body surface area, Fick’s principle, and per body weight. The CO obtained by the BSA was greater (p = 0.0001, ANOVA, Tukey) than that obtained by the other methods. We conclude that although the methods used in this study to estimate CO are reliable, there are significant differences between them; therefore, each method must be evaluated by the investigator to determine which meets the needs of the protocol.
Introduction
In lung transplantation centers, ex vivo lung perfusion (EVLP) is a tool that helps increase the potential for donation of lungs that do not meet the standard criteria for transplantation1. This is achieved by preserving and improving the lung functionality of donors with brain death or cardiac arrest, as well as by evaluating lung performance before transplantation2,3,4. In EVLP, an extracorporeal circulation pump allows perfusion of the lung to be transplanted through a membrane gas exchanger and a leukocyte trapping filter5.
To date, several EVLP protocols have been described (Toronto, Lund, and Organ Care System). These are differentiated by the type of perfusion solution used, whether the left atrium is kept open or closed during perfusion, and by the perfusion flow, which varies from 40% to 100% (depending on the technique used) of the estimated cardiac output (CO) of the donor6,7,8. CO is the amount of blood pumped by the heart per minute9 and is the mechanism by which tissue perfusion is maintained. Thus, CO monitoring ensures proper tissue oxygenation. CO, a product of the heart rate and the stroke volume, is measured in liters10,11,12. However, this approach for maintaining tissue perfusion also depends on other factors, such as venous return, peripheral oxygen use, systemic vascular resistance, respiration, total blood volume, and body position12.
There are several devices for measuring and monitoring CO, some of which use simple physical principles, while others use mathematical models. These methods include the Fick principle, thermodilution (transpulmonary or lithium dilution), analysis of the arterial pressure wave to estimate stroke volume (SV), and less invasive methods such as Doppler or thoracic bioreactance. However, no CO monitoring device can meet all clinical requirements due to the limitations of the corresponding monitoring technique10,13.
The measurement of CO by transcardiac thermodilution is a simple and easily reproducible method in pigs. It involves placing a catheter with a thermistor in the pulmonary artery and injecting a volume of liquid with a temperature lower than that of the blood. The thermistor detects changes in temperature over time, which are then plotted in the form of a curve, with the area under the curve representing minute volume14. Various studies have described that for EVLP animal models, CO can be calculated by weight (100 mL/kg)15, thermodilution, and Fick's method10,13. However, in the clinic, CO is calculated using the cardiac index (CI), which is the CO adjusted to the donor's body surface area16. Nevertheless, there are no studies comparing these methods in experimental pig models.
The objective of this study was to reproduce the measurement of CO by thermodilution in pigs and compare its precision and accuracy with those obtained using CO adjusted by BSA, weight, and Fick's method to establish perfusion flow during EVLP.
Protocol
The protocol (B09-17) was approved by the bioethics committee of the INER (Instituto Nacional de Enfermedades Respiratorias "Ismael Cosio Villegas"). Twenty-three clinically healthy Landrace pigs of either sex, weighing between 20-25 kg, were used for this study. The animals were handled according to the technical specifications for the Care and Use of Laboratory Animals of the Official Mexican Standard17 and the Guide for the Care and Use of Laboratory Animals of the USA18. All animals were obtained from the Instituto Nacional de Enfermedades Respiratorias Ismael Cosio Villegas and were housed in individual cages under identical environmental conditions, provided with water and food ad libitum. In all animals, a thermodilution catheter was placed in the right jugular vein, and an arterial catheter was placed in the carotid artery on the same side to collect blood gases and then calculate the CO. The details of the reagents and equipment used are listed in the Table of Materials.
1. Experimental preparation
- Dilute 1000 IU of heparin in each of three 250 mL 0.9% sodium chloride solutions (saline solution, SS).
- Attach pressure transducers to the vital signs monitor. Use each transducer to measure the pressure at the corresponding port of the thermodilution catheter.
- Connect the heparinized solutions to the transducer via needleless intravenous infusion. Ensure they are cleared and ready to connect to the catheter.
- Remove the thermodilution catheter from the packaging. Immerse the distal end in 0.9% NaCl to check the integrity of the balloon.
- Check the patency of the distal and proximal catheter connections. Keep the catheter on the surgical instrument table until use.
2. Animal preparation
- Administer 0.05 mg/kg atropine and 4 mg/kg tiletamine-zolazepam intramuscularly to all pigs in the animal preparation room (following institutionally approved protocols).
- Leave the pigs undisturbed but under surveillance until they become recumbent and remain in this position without signs of excitement or response to nociceptive stimuli.
- Place the sedated animal in the prone position and insert a catheter into the marginal vein of the left ear.
- Transfer the animal to the operating room for surgery.
- Place the animal in the dorsal position and administer 4 mg/kg propofol IV, 300 µg/kg vecuronium bromide, and 0.1 mg/kg fentanyl IV.
- Lower the mandible of the pig with the help of laboratory staff to keep the mouth open and the tongue sticking out.
- Spray 10% lidocaine onto the vocal cords, clear accumulated saliva with gauze held by ring forceps, and separate the epiglottis from the laryngeal opening.
- Identify the tracheal entrance with a laryngoscope and a number 3 straight blade, then insert a 7 Fr endotracheal tube with a balloon.
- Inflate the balloon and fix the tube to the mandible after verifying its placement within the airway.
- Connect the pig to the anesthesia machine to maintain an anesthetic state with 2.5%-3% sevoflurane (Figure 1).
- Ventilate the animal in volume-controlled ventilation mode with a frequency of 25 breaths/min, tidal volume of 6-8 mL/kg weight, FiO2% of 50%-70% to maintain SaO2 greater than 90%, trigger of 2, positive end-expiratory pressure (PEEP) of 5 cmH2O, inspiration ratio of 1:2 s, and inspiratory flow of 15 L/min and maximum of 30 L/min.
3. Placement of the thermodilution catheter and measurement of cardiac output
- Keep the animal in the dorsal position under general anesthesia and perform antisepsis of the cervical region with iodopovidone (Figure 2). Make a 10 cm paramedian incision using an electrocautery pencil and dissect the subcutaneous tissue to expose the right external jugular vein by blunt dissection.
- Place two 2-0 silk sutures, one at the distal portion and the other at the proximal portion of the dissected vessel (Figure 3).
- Insert the catheter extracorporeally from the neck site to the thoracic region where the heart is located. Measure the insertion depth using markings on the catheter to reach the pulmonary artery (PA). Ligate the distal portion of the vessel and place a double loop in the proximal portion to secure the catheter once inserted.
- Make a 2 mm transverse incision on the ventral portion of the vessel using iris scissors. Open the edges of the incision with Halsted's mosquito hemostatic forceps and insert the 5Fr thermodilution catheter into the right jugular vein (Figure 4, Figure 5, and Figure 6). Direct the catheter towards the pulmonary artery (PA) by following the curves displayed on the monitor.
4. Placement of the arterial catheter
- Once the vein is dissected and reference sutures are placed, displace the sternocephalic muscle (equivalent to the sternocleidomastoid) laterally.
- Dissect the pretracheal (sternohyoid) musculature until the carotid artery is exposed.
- Cannulate the carotid artery similar to the jugular vein and connect it to the pressure transducer for monitoring the systemic arterial pressure.
5. Evaluation
- Once the thermodilution catheter is placed in the right jugular vein and the arterial catheter is placed in the carotid artery on the same side, take samples for blood gas analysis.
- Obtain the blood gas values and evaluate cardiac output (CO) using the thermodilution method, body surface area, and Fick's method.
NOTE: For detailed procedures, please refer to previously published reports19–21.
6. Statistical analysis
- Analyze data demonstrating a normal distribution using analysis of variance (ANOVA) and perform Tukey's post hoc test. Express values as the mean ± standard error. Consider p values <0.05 as indicating statistical significance.
7. Thermodilution measurement
- Inject a 5 mL bolus of cold SS at 4 °C into the proximal lumen of the thermodilution catheter in less than 4 s.
- Observe the thermodilution curve (temperature/time) on the monitor screen. The curve should show a rapid ascent followed by a smooth and gradual descent to the baseline, with numerical values displayed with one or two decimal places.
- Repeat the bolus injection process with two additional boluses of cold SS until the curves are valid, similar, and within 10% of the average value.
- After confirming the validity and similarity of the curves, calculate the average of the three values and record it as the final CO value in liters per minute. Obtain CO and other indices from the thermodilution curve using calculations based on the Stewart-Hamilton equation21.
8. Determining adjusted cardiac output for body surface area (BSA) or cardiac index
- To determine the adjusted cardiac output (CI), calculate the body surface area (BSA) using the DuBois-DuBois formula19:
BSA = 0.007184 × (Height (cm)0.725) × (Weight (kg)0.425). - Once BSA is obtained, calculate the CI using the formula20:
CI = CO/BSA.
NOTE: CO is determined in step 7.
9. Estimating cardiac output by the Fick's method
- To calculate cardiac output (CO) using the Fick's method, determine the oxygen consumption (VO2) and the difference in oxygen levels obtained from arterial (SaO2) and venous (SvO2) blood gases. Calculate VO2 using the formula21:
VO2 = CO x (SaO2 – SvO2). - Then, determine cardiac output using the formula21:
CO = VO2 / ([SaO2 – SvO2] × 10).
10. Estimating cardiac output per body weight
- Determine the cardiac output per bodyweight of the animals following previous reports8,15.
NOTE: In the EVLP protocol, various groups have reported that the estimated cardiac output (CO) per body weight in pigs is 100 mL/kg8,15.
11. Euthanasia
- Euthanize all animals with an overdose of sodium pentobarbital (150 mg/kg/IV) via the jugular vein sheath (following institutionally approved protocols) once all measurements are completed.
- Continue general anesthesia and cardiac monitoring until the electrocardiography (ECG) trace shows no cardiac electrical activity17,18.
Representative Results
All animals survived the surgical procedure and the study time. One animal (4.3%) developed a jugular vein tear due to excessive traction during catheter insertion. Furthermore, none of the intervened vessels showed bleeding. In the studied animals, an average of 25-30 cm of catheter insertion was required to reach the PA. In three cases (13%), the catheter was directed towards the right upper limb of the pig. In these cases, the catheter was retracted to the insertion site, the pig's upper limb was repositioned towards its head, and the jugular vein was manually occluded to guide the catheter toward the heart. Two animals (8.6%) developed tachycardia and arrhythmias during catheter insertion. These resolved on their own and did not require pharmacological management. When comparing the CO obtained by the four methods, the value adjusted by the body surface area (p < 0.05; ANOVA, Tukey) was greater than that obtained with the thermodilution method and the CO adjusted by weight (Figure 7).

Figure 1: Intubation and anesthesia setup. Pig intubated and connected to an inhaled anesthesia machine. Please click here to view a larger version of this figure.

Figure 2: Antisepsis of the cervical region. Please click here to view a larger version of this figure.
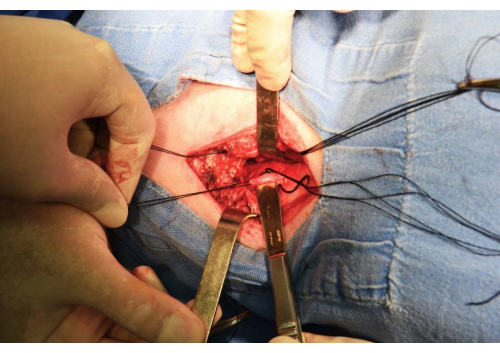
Figure 3: Jugular vein dissection. The jugular vein dissected and reference sutures placed around it. Please click here to view a larger version of this figure.
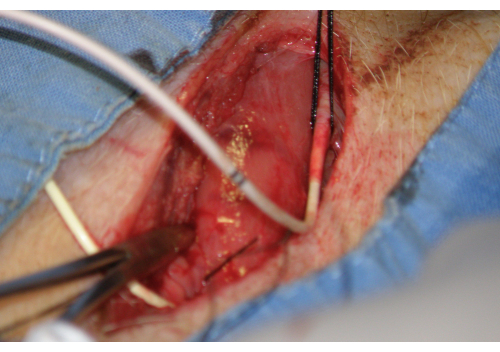
Figure 4: Catheter insertion. Insertion of the catheter into the transverse incision in the ventral portion of the jugular vein. Please click here to view a larger version of this figure.
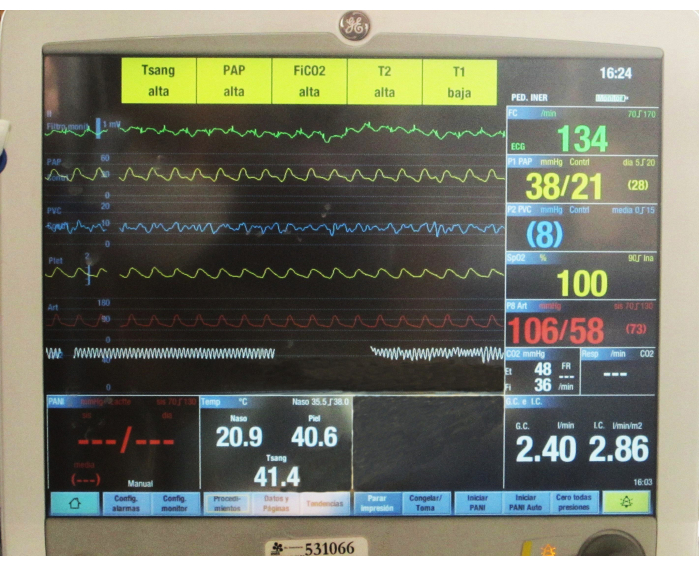
Figure 5: Thermodilution catheter insertion tracing. Normal insertion tracing during thermodilution catheter placement. Please click here to view a larger version of this figure.
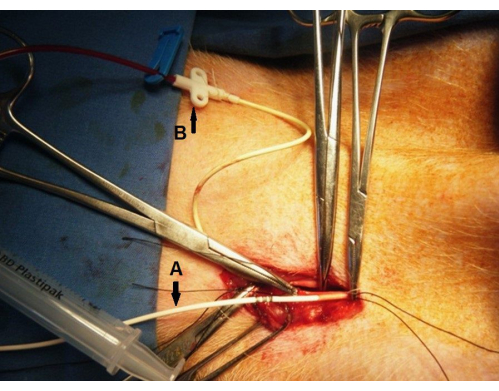
Figure 6: Final catheter placement. End of catheter placement in the jugular vein (A) and carotid artery (B). Please click here to view a larger version of this figure.
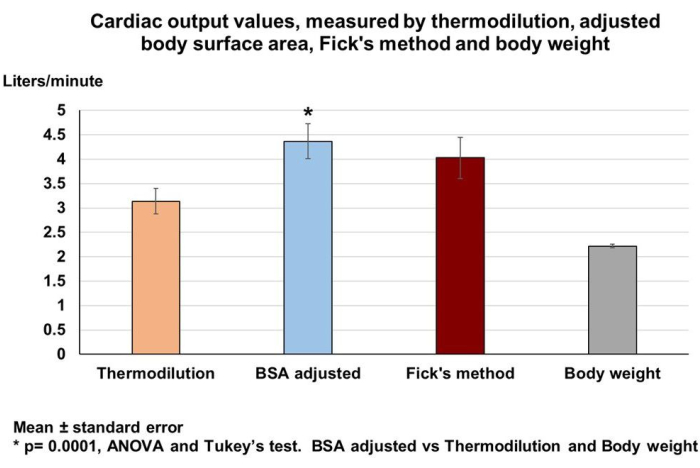
Figure 7: Cardiac output estimation. Highest cardiac output (mean ± standard error) estimated by the adjusted body surface area method. Please click here to view a larger version of this figure.
Discussion
EVLP in pigs has a direct translation to human clinical practice, given the comparability in the size, physiology, and genomic sequence of the two species22. According to the EVLP protocol selected by the researcher, the measurement of CO is essential for determining the flow required to perfuse the lungs. Moreover, depending on the resources and knowledge available, the appropriate method can be chosen. However, no study has compared the methods for evaluating CO simultaneously against a reference method. Therefore, this study was designed to compare four techniques for measuring CO to estimate pulmonary flow during EVLP. We included two techniques typically used in experimental hemodynamic laboratory studies and two techniques that employ calculated cardiovascular parameters used in clinical care. This study showed that in healthy pigs, when the four techniques were directly compared, the value produced by the adjusted BSA method was significantly different.
The reference method, thermodilution, offers quick, easy, and instantaneous measurements; therefore, if one has access to measurement and data acquisition instruments, and depending on the needs of the protocol, thermodilution catheters are ideal. Additionally, this method is based on simple physical principles and is very precise since it uses indicators that indirectly quantify blood flow23. This method was first described in 1970; after injecting a predetermined volume of cold saline into the proximal port of a pulmonary artery catheter, the thermal variations in the blood are measured. In this study, open vascular dissection was used for cannulating the jugular vein and carotid artery due to the ease of visibility when incising the skin and separating the neck muscles, which has led to the routine use of this technique in our laboratory. It is worth mentioning that the Seldinger technique can be used in this experimental model; however, in addition to requiring additional equipment, in our experience, this technique is difficult to perform in pigs if one lacks sufficient training.
The advantages of the thermodilution technique include its reliability and the ease of performing serial measurements without the need to obtain blood samples, as required for Fick’s method23. On the other hand, the calculated cardiovascular parameters are important clinical tools that complement direct measurements when evaluating the state of the cardiovascular system. The CI is used to show how CO and BSA are correlated. This derived cardiovascular index is important and easy to calculate, which makes it attractive for use in decision-making in settings with limited resources20. However, in this study, the BSA method yielded significantly greater values than the other methods, which may indicate an overestimation of pulmonary perfusion flow when compared with the flow obtained using the other methods.
Fick’s measurement of cardiac output was first described in 1870 as a method for measuring CO in humans. Fick postulated that the total uptake or release of oxygen by the lungs is the product of blood flow through the lungs and the arteriovenous difference in blood oxygen. This technique is used in cardiac catheterization laboratories because it is very precise and provides information on numerical trends based on mathematical models; however, it is not practical for use in clinical settings or for continuous measurement of CO21,24.
Regarding the CO obtained by the weight method, we found that this value is lower than those of the other methods, but it could be useful for those who perform EVLP in pigs. As described by Beller et al.8, who compared EVLP with flows of 20% of the predicted CO, it was found that this approach improved lung function, reduced edema, and attenuated inflammation after transplantation.
Finally, the literature indicates that the different CO monitoring techniques have their own limitations and that no device can meet all practice requirements. However, depending on the needs of the researcher, if there is limited access to advanced measurement tools, the determination of CO by calculation is also reliable, simple, reproducible, and requires less time than invasive techniques2,20. Although these methods for estimating CO are reliable, there are significant differences among them. Therefore, each method must be evaluated by the researcher to determine which one meets the needs of their protocol.
It needs to be mentioned that this study has a limitation because a comparison with other widely used CO measurement techniques, such as Doppler technology (transthoracic, transesophageal, and echocardiography) or bioimpedance-thoracic electrical bioreactance, was not included here. Including these methods could provide valuable insight into the agreement between these techniques and pulmonary artery catheterization (PAC) for CO measurement in pigs.
Disclosures
The authors have nothing to disclose.
Acknowledgements
The authors want to thank Roberto, Rueda, and Sergio Martínez for their invaluable technical assistance with technical support with animals.
Materials
| Anesthesia machine | General Electric | Carescape 620 | |
| Atropine | Amixteria, Stern Pharma GmbH | ||
| Catheter Insyte Autoguard 20 GA | Becton Dickinson | 381434 | |
| Electrocautery pencil | BBraun Aesculap | GN211 | |
| Endotracheal tube with a 7 Fr balloon | Rush | MG 027770 002 | |
| Fentanyl | Janssen-Cilag | ||
| Iodopovidone | Degasa | NDC6732635208 | |
| Laryngoscope | Riester | ||
| Lidocaine Spray | Pisa | ||
| Pressure transducers | Edwards Lifesciences | PX260 | |
| Propofol | Pisa | ||
| Sevofluorane | Pisa | ||
| Silk sutures 2-0 | Covidien | GS833 | |
| Sodium pentobarbital | Pfizer | ||
| straight blade of laryngoscope #3 | Miller; Riester | ||
| Swan-Ganz 5Fr thermodilution catheter | Arrow Thermodilution Ballon Catheter | Ref AI-07165 | |
| Tiletamine-zolazepam | Virbac | ||
| Vecuronium bromide | Pisa |
References
- Mohite, P. N., et al. Ex vivo lung perfusion made easy. Multimed Man Cardiothorac Surg. 23, 2021 (2021).
- Cypel, M., Keshavjee, S. Ex vivo lung perfusion. Oper Tech Thorac Cardiovasc Surg. 19 (4), 433-442 (2014).
- Langmuur, S. J. J., Max, S. A., Çelik, M., Mahtab, E. A. F. Ex vivo lung perfusion: A procedural guide. Multimed Man Cardiothorac Surg. 2023, (2023).
- Kesseli, S. J., Davis, R. P., Hartwig, M. G. Commentary: Making lungs great again-introducing new modifications to the Toronto ex vivo lung perfusion protocol. J Thorac Cardiovasc Surg. 161 (6), 1974-1975 (2021).
- Roman, M. A., Nair, S., Tsui, S., Dunning, J., Parmar, J. S. Ex vivo lung perfusion: A comprehensive review of the development and exploration of future trends. Transplantation. 96 (6), 509-518 (2013).
- Van Raemdonck, D., Neyrinck, A., Cypel, M., Keshavjee, S. Ex-vivo lung perfusion. Transpl Int. 28 (6), 643-656 (2015).
- Machuca, T. N., Cypel, M. Ex vivo lung perfusion. J Thorac Dis. 6 (8), 1054-1062 (2014).
- Beller, J. P., et al. Reduced-flow ex vivo lung perfusion to rehabilitate lungs donated after circulatory death. J Heart Lung Transplant. 39 (1), 74-82 (2020).
- García, X., et al. Estimating cardiac output, utility in the clinical practice: Available invasive and non-invasive monitoring. Med Intensiva. 35 (9), 552-561 (2011).
- Blanco-Tencio, F. M. . Comparability of cardiac output measured by pulse contour analysis compared with transesophageal echocardiography at the Calderón Guardia Hospital from April to July 2021. Tesis Especialidad en Anestesiología y Recuperación. , (2021).
- Physiology, Cardiac output. StatPearls. StatPearls Available from: https://www.ncbi.nlm.nih.gov/books/NBK470455/ (2022)
- Johnson, B., et al. Cardiac physiology. Essentials of Cardiac Anesthesia. , 53-66 (2008).
- Corsini, A., Cercenelli, L., Zecchi, M., Marcelli, E., Corazza, I. Basic hemodynamic parameters. Advances in Cardiovascular Technology. , 463-474 (2022).
- Mateu Campos, M. L., et al. Techniques available for hemodynamic monitoring: Advantages and limitations. Med Intensiva. 36 (6), 434-444 (2012).
- Cypel, M., et al. Technique for prolonged normothermic ex vivo lung perfusion. J Heart Lung Transplant. 27 (12), 1319-1325 (2008).
- National Transplant Organization. National protocol for the maintenance of potential donor in brain death. SEMICYUC. , (2020).
- Estados Unidos Mexicanos. AFÍA. Especificaciones Técnicas para la Producción, Cuidado y Uso de Animales de Laboratorio de la Norma Oficial Mexicana NOM-062-ZOO-1999. Diario Oficial de la Federación 6 dic. , (1999).
- National Institutes of Health U.S.A. Guía Para el Cuidado y Uso de Los Animales de Laboratorio. Department of Health and Human Services, Public Health Service, National Institutes of Health U.S.A. Edición Mexicana Auspiciada por la Academia Nacional de Medicina. , (2002).
- Flint, B., Hall, C. A. Body surface area. StatPearls. , (2023).
- Ewah, P. A., Oyeyemi, A. Y. Relation between derived cardiovascular indices, body surface area, and blood pressure/heart rate recovery among active and inactive Nigerian student. Bull Fac Phys Ther. 27, 34 (2022).
- Kobe, J., et al. Cardiac output monitoring: Technology and choice. Ann Card Anaesth. 22 (1), 6-17 (2019).
- Nelson, K., et al. Animal models of ex vivo lung perfusion as a platform for transplantation research. World J Exp Med. 4 (2), 7-15 (2014).
- Argueta, E., Paniagua, D. Thermodilution cardiac output a concept over 250 years in the making. Cardiology Rev. 27 (3), 138-144 (2019).
- Perry, D. A., et al. Changes in tissue oxygen tension, venous saturation, and Fick-based assessments of cardiac output during hyperoxia. Acta Anaesthesiol Scand. 63 (1), 93-100 (2019).

.