Spinal cord compression injury and loss of function
As described previously, by optimizing the preoperative, surgical and postoperative procedures, a reproducible compression SCI model in the neonatal mouse can be obtained1. The polyethylene stopper placed on one blade of the clip (Figure 2B and C) prevents the full closure of the clip and keeps the inter-blade distance consistently at about 230 µm. Reversing the orientation of the clip in between the two compressions results in a symmetrical injury, as judged by histological sequelae (Figure 5A and 1). Immediately after mini-clip removal, the compressed spinal cord tissue becomes darker due to hemorrhagic contusion and edema. Observation of serial sections of the injured spinal cord stained for Eosin and Hematoxylin already one day after injury reveals gradual deterioration of the tissue when approaching the lesion epicenter (Figure 5A). The presence of intraspinal cavities or blood in the lesion is not unusual.
Behavioral assessment, for example by tracking hindlimb trajectories under non-weight bearing conditions a few hours after surgery, shows a dramatic impairment of hindlimb motility in SCC injured mice compared to sham control mice in which only a laminectomy is performed (Figure 5B and 1). This test can be repeated until the mouse is able to perform other behavioral tests that require bearing its own weight1.
Mortality and recovery after surgery
Intraoperative mortality is mainly due to apnea and cardiac arrest caused by the high concentration of isoflurane needed to achieve sufficient anesthesia. Introducing the local anesthetic Bupivacaine into the surgical protocol permits reduction of the isoflurane concentration and thereby diminishes significantly the mortality rate. In a recent experimental series including more than 20 animals, the intraoperative mortality was nil. In contrast, post-operative survival is mainly influenced by the acceptance of the operated mice by their mother. A significant improvement occurred when anxiety and aggressiveness was reduced by delivering a single injection of Diazepam (i.p. 8 g/kg body weight) to the mother before returning the operated mice to the litter1. Acceptance and postoperative recovery of the operated mice can be monitored by the presence of milk in the stomach. The stomach of a P1-P7 mouse that has drunken milk is clearly white and visible through the abdominal skin (Figure 3). Comparison of feeding in operated, sham control and unoperated mice is useful for assessing the nutritional status of injured mice. Assessing the growth of operated versus unoperated mice shows that despite a little weight loss during the first post-operative day, the growth curve of operated mice normalizes rapidly thereafter (Figure 6). Mortality related to bladder dysfunction or infection was never observed even in mice studied for as long as 7 weeks.
| Number in Fig. 2 | Name | Manufacturer/Provider | Reference # | Link | Comment | ||
| 1 | Plastic syringe (30 or 50 ml) | ||||||
| 2 | Plastic Petri dish (150 x 25 mm) | ||||||
| 3 | Fortec isoflurane vaporizer | Cyprane | http://www.mssmedical.co.uk/products/new-vaporisers/ | We use and old device out of production, check the link for newer device | |||
| 4a | Yasargil temporary aneurysm mini-clip | Æsculap | FE681K | http://www.aesculapusa.com/assets/base/doc/DOC697_Rev_C-Yasargil_Aneurysm_Clip.pdf | |||
| 4b | Fine bore polyethylene capillary tubing ID 0.58 mm, OD 0.96 mm | Smiths Medical | 800/100/200 | http://www.smiths-medical.com/industrialproducts/8/39/ | |||
| 5 | Isoflurane (Forene) | Abbott GmbH & Co. KG | http://www.life-sciences-europe.com/product/forene-abbott-gmbh-wiesbaden-group-narcotic-germany-west-2001-1858.html | ||||
| 6 | Marcain (Bupivacain) | AstraZeneca | http://www.astrazeneca.co.uk/medicines01/neuroscience/Product/marcaine | ||||
| 7 | Insuline syringe 0.3 ml 30 G x 8mm | VWR | 80086-442 | https://us.vwr.com/store/catalog/product.jsp?product_id=4646138 | |||
| 8 | Ultra Fine Micro Knife 5 mm cutting edge | Fine Science Tools | 10315-12 | http://www.finescience.de/katalog_ansicht.asp?Suchtyp= Kat&suchkatalog=0019900000&reloadmenu=1 |
|||
| 9 | Extra Fine Graefe Forceps — 0.5 mm Tip | Fine Science Tools | 1153-10 | http://www.finescience.de/katalog_ansicht.asp?Suchtyp= Kat&suchkatalog=0055700000&reloadmenu=1 |
Not really necessary, often the teeth are too large | ||
| 10 | Forceps SuperGrip Straight | Fine Science Tools | 00632-11 | http://www.finescience.de/katalog_ansicht.asp?Suchtyp= Kat&suchkatalog=0053500000&reloadmenu=1 |
Two forceps are necessary | ||
| 11 | Spongostan Special 70 x 50 x 1 mm | Ferrosan | |||||
| 12 | Vannas Spring Scissors — 2 mm Blades Straight | Fine Science Tools | 15000-03 | http://www.finescience.de/katalog_ansicht.asp?Suchtyp= Kat&suchkatalog=0012800000&reloadmenu=1 |
|||
| 13 | Vario Clip Applying Forceps | Aesculap | FE502T | http://www.aesculapusa.com/assets/base/doc/DOC697_Rev_C-Yasargil_Aneurysm_Clip.pdf | |||
| 14 | Vicryl 6–0 (Ethicon) | Johnson and Johnson | J105G | ||||
| 15 | Diethrich micro needle holder | 11-510-20 | http://trimed-ltd.com/Products/Suture-Instruments/Micro-Needle-Holders-With-Tungsten-Carbide-Inserts/Ref-11-29.html | ||||
| 16 | Temgesic (buprenorphine) | Schering-Plough | |||||
| 17 | Stesolid (diazepam) | Actavis | Also known as Valium | ||||
| 18 | Pedamix | Fresenius Kabi | http://www.helsebiblioteket.no/retningslinjer/pediatri/mage-tarm-lever-ern%C3%A6ring/parenteral-ern%C3%A6ring | ||||
| 19 | Klorhexidinsprit (chlorhexidine gluconate) | Fresenius Kabi | D08A C02 | http://www.felleskatalogen.no/medisin/klorhexidinsprit-fresenius-kabi-klorhexidinsprit-farget-fresenius-kabi-fresenius-kabi-560639 | |||
Table 1. List of tools and equipment for generating a clip-driven spinal cord compression injury in a neonatal mouse.
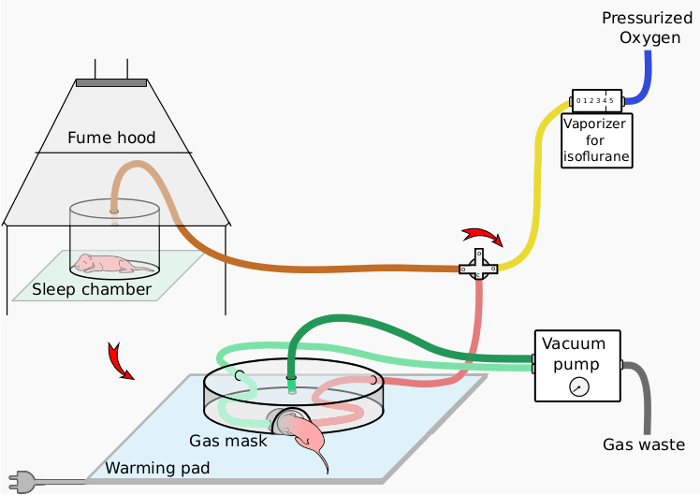
Figure 1. Schematic of anesthesia setup. This schematic presents the anesthesia setup designed for the neonatal mouse, with a sleep chamber for initial anesthesia and a nose mask device for continued anesthesia during surgery.
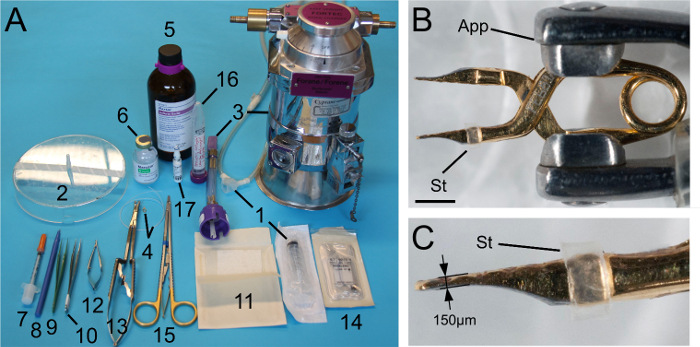
Figure 2. Principal tools and compression clip. (A) Tools used during the procedure. The numbers correspond to the annotation used in Table 1. (B and C) A Yasargil temporary aneurysm mini-clip with the tip of each blade manually trimmed down to about 150 µm thickness. A stopper made of a slice of polyethylene tubing (Table 1) is placed on one of the blades to prevent full closure of the clip. Scale bar: 2 mm. App: clip applicator (#12 in A); St: stopper. Please click here to view a larger version of this figure.
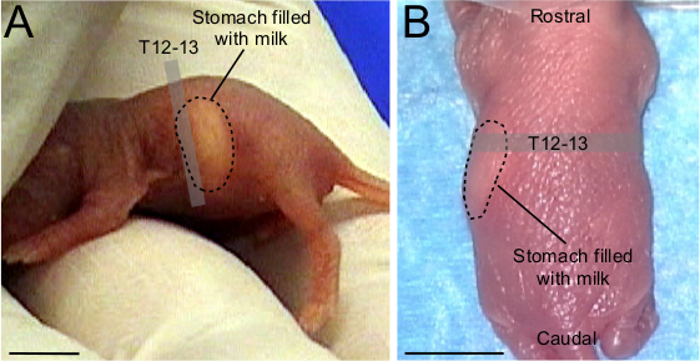
Figure 3. Landmark for preoperative assessment of spinal level in neonatal ICR mouse. (A) Lateral view of a P1 ICR mouse with white milk in the stomach. The rostral part of the stomach corresponds to T12-T13 spinal level. (B) P1 ICR mouse under anesthesia in a prone position. Although more difficult to visualize than in (A), the stomach filled with milk is recognizable. The rostral part of the stomach indicates T12-T13 spinal level. Scale bars: 0.5 cm.
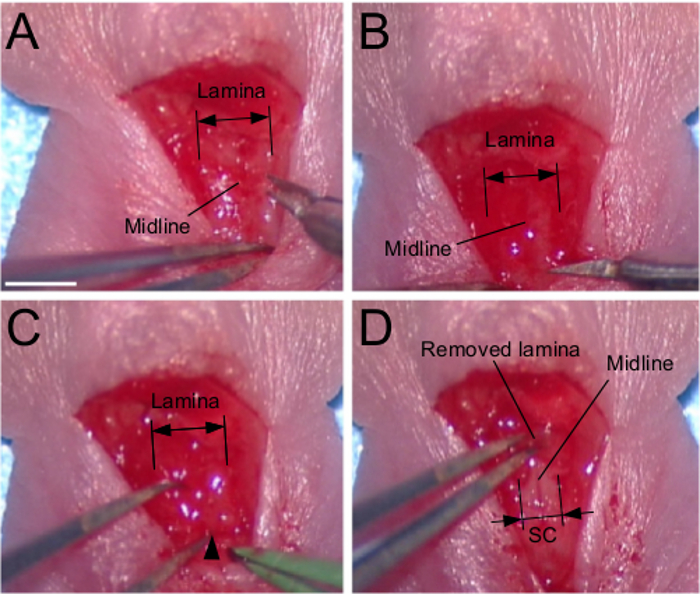
Figure 4. Dorsal laminectomy. (A) Dissection of paravertebral muscles. Note that at this age the spinal process is underdeveloped. (B) Transversal sectioning of the lamina with thin scissors. (C) Introduction of one blade of a thin forceps between the lamina and the dura. The entry point is shown by the arrowhead. (D) Removal of the lamina. Scale bar: 2 mm.
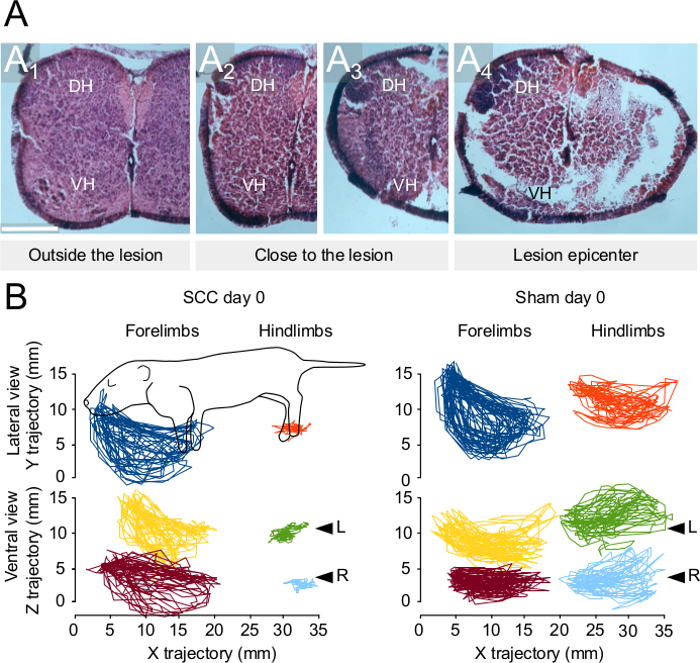
Figure 5. Histological and behavioral outcomes after spinal cord compression injury at P1. (A) Eosin and Hematoxylin staining in spinal cord sections from an injured mouse (1 day after injury) at different distance from the injury epicenter. (B) Representative traces of forelimb and hindlimb trajectories observed 6 hours after injury or after a sham control laminectomy. Traces on the top represent trajectories viewed from a lateral view of the animal. Traces at the bottom represent trajectories viewed from the ventral aspect of the animal. See also 1. Scale bar: 250 µm. DH: dorsal horn; L, left; R: right; SCC: spinal cord compression; VH: ventral horn. Please click here to view a larger version of this figure.
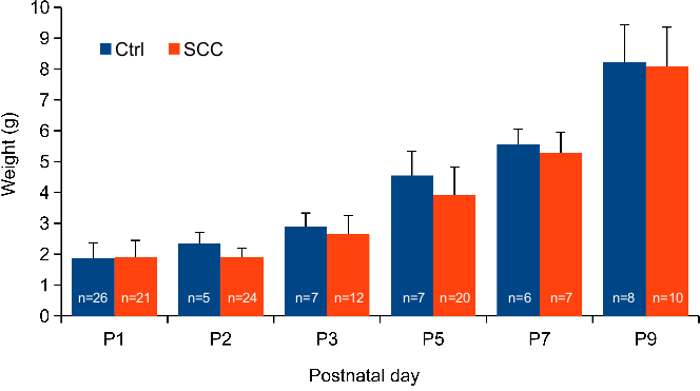
Figure 6. Comparative growth curves. Histogram showing the weight gain of unoperated and SCC injured mice from postnatal day 1 to postnatal day 9.
