The passive transfer of antigen specific antibodies results in a full blown disease in mice, resembling at clinical, histological and immunopathological levels the human EBA. Blisters, crusts, erosions and alopecia develop on the ears, snout, paws, legs, back and around the eyes of the mice. The first clinical signs of the disease will most probably appear on the ears and/or head area. Deposition of specific rabbit IgG, and mouse complement C3 is detected by direct IF at the dermal epidermal junction in cryosections of perilesional skin. In lesional skin subepidermal blisters and inflammatory infiltrate are seen by histology.
However, if the injection of pathogenic collagen VII-specific antibodies is discontinued, the disease activity gradually becomes lower, and within several weeks the lesions heal. Nevertheless, a certain degree of postinflammatory cicatricial alopecia may persist indefinitely.
Characterization of the recombinant autoantigen (and of pathogenic IgG)
Murine collagen specific IgG binds at the dermal -epidermal junction (Figure 2B). The specificity is assessed by immunoblot (Figure 2C, lanes 3, 4 and 7).
Scoring disease activity
The clinical evaluation of the disease is based on a scoring system we developed (Table 1): 0, no lesions; 1, less than 1% of the skin surface; 2, 1-5% of the skin surface; 3, 5-10% of the skin surface; 4, 10-20% of the skin surface is affected. IgG against murine collagen VII induces cutaneous lesions such as erythema, alopecia, blisters, erosions, crusts on the ears, eyes, snout, limbs and trunk of Balb/c mice (Figure 3).
Analysis of tissue-bound and circulating collagen-specific antibodies
Deposition of rabbit IgG, and mouse complement C3 are detected in frozen, perilesional tissue sections (Figure 4D and E respectively). The subepidermal blisters and the inflammatory infiltrate are seen in histological samples (Figure 4F). Circulating rabbit antibodies are analyzed by ELISA (Figure 5). Frozen tissue and/or organ extracts are analyzed by different assays for their protein and enzyme content (MPO assay).
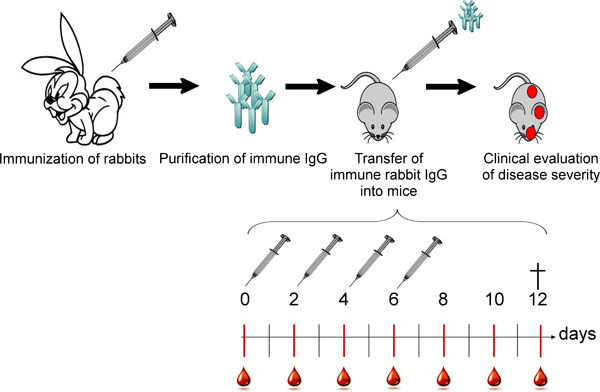
Figure 1. Overall scheme of the in vivo blistering induced by the passive transfer of collagen VII-specific antibodies. Rabbits are immunized with murine collagen VII and rabbit IgG is purified from the immune sera. Subsequently, the specific autoantibodies are injected subcutaneously into mice following an injection/bleeding schedule. Mice are being checked for general health condition and disease signs daily.
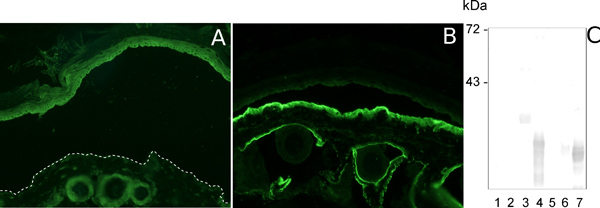
Figure 2. Characterization of pathogenic collagen VII-specific IgG. Indirect IF analysis of salt-split normal mouse skin sections incubated with pre-immune rabbit serum and with murine collagen VII-specific immune rabbit serum results in no deposition (A) and deposition of autoantibodies at the dermal epidermal junction (B), respectively. The specific antibodies recognize the antigen(s) they were raised against when immunoblot with a set of overlapping recombinant murine collagen VII fragments is performed (C, lanes 3, 4 and 7).
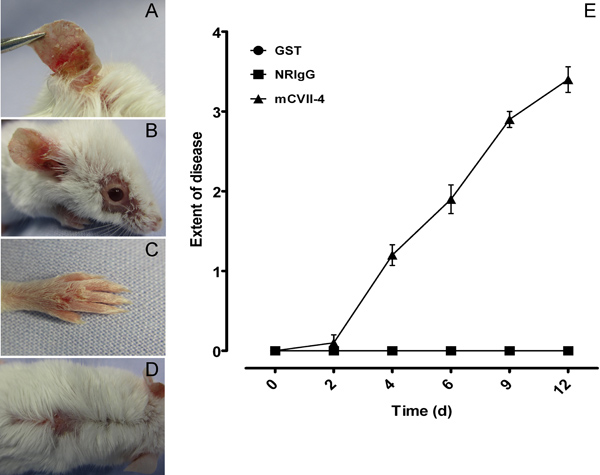
Figure 3. Clinical evaluation of mice. IgG to murine collagen VII induces cutaneous lesions such as alopecia, blisters, erosions, crusts on the ears, eyes, snout, limbs and trunk of Balb/c mice (A-D). Mice injected with specific autoantibodies reach a score of 4, whereas the ones injected with NRIgG or Abs against an indifferent protein had a score of 0 (E). The clinical score was calculated as follows: 0, no lesions; 1, less than 1% of the skin surface; 2, 1-5% of the skin surface; 3, 5-10% of the skin surface; 4, 10-20% of the skin surface is affected. Weight loss of 5-10% of the total body weight during three consecutive days counts as an extra point in the final score.
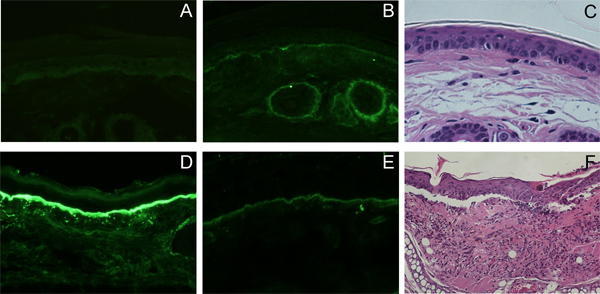
Figure 4. Histo- and immunopathological findings in mice injected with collagen VII-specific IgG. Deposition of rabbit IgG (D), and mouse complement C3 (E) is detected by direct IF at the dermal epidermal junction in cryosections of perilesional skin, in vivo. In lesional skin subepidermal blisters and inflammatory infiltrate is seen by histology (F). No deposition of rabbit IgG (A), mouse complement C3 (B), nor is subepidermal blister formation seen in the controls (C).

Figure 5. Immunoassay of plasma from mice injected with collagen VII-specific IgG. Plasma levels of circulating rabbit antibodies were measured by ELISA.

Table 1. Skin blistering disease scoring sheet. Click here to view larger table.
Scoring system:
- 0, no lesions;
- 1, less than 1% of the skin surface;
- 2, 1-5% of the skin surface;
- 3, 5-10% of the skin surface;
- 4, 10-20% of the skin surface is affected.
Extra hints when scoring:
- Weight loss of 5-10% of the total body weight during three consecutive days counts as an extra point in the final score 17.
- Erythema on the ears, around the eyes on paws are just the first signs of an ongoing immune reaction, if not paired with blisters or alopecia they are not quantified, just taken under observation.
- Marks on the tail could be bite or fight marks, so if they are present from the beginning their worsening might not necessarily be due to the disease. Consider carefully weather to count them!
