1. Setup: Aseptic Technique11
- Turn on Laminar Flow Hood (LFH).
- Turn on the Nitrogen gas control unit. Ensure that hose is connected between console unit and Nitrogen tank. Turn gas on. Gas setting should be set to 50-60 PSI on regulator tank. Turbine pressure on unit should read 3.3 to 3.4 Bars.
- Press Test button. Atmospheric pressure will read in the 700s and pumps 1 and 2 should be below 200. The unit will beep when testing is complete. Don mask with eye protection, as applicable, and cap. Wash hands and don non-sterile gloves. Place sterile kits inside LFH and open wraps to establish sterile field.
- Place one sterile medicine cup and one sterile plastic basin with sterile gauze next to the established sterile field. Pour sterile isopropyl alcohol into medicine cup. Wipe pachymetry probe with alcohol swab/pad and place probe, tip down, into medicine cup. The probe tip should soak in isopropyl alcohol for 10 minutes. After pachymetry probe has soaked for 10 minutes, rinse the probe tip with sterile water from the prefilled syringe to remove alcohol and place probe in the plastic basin.
- Using aseptic technique, open and drop sterile items (blade, sterile gloves, and corneal viewing chambers) onto sterile field unless already part of the pre-made pack.
- Obtain corneal tissue in preservation media and place inside LFH (Figure 2).
- Open vial(s) and dispose of the lid(s) into an appropriate biohazard receptacle. Discard non-sterile gloves.
- Don sterile gloves. Place pre-packed plastic basin to the side of the field where pachymeter is located. Connect infusion line to stopcock and place spike end of infusion line outside of hood securing the line in such a way as to prevent the line outside of the hood from reentering the hood and touching the sterile field.
- Perform corneal tissue transfer. Gently pour the tissue and medium, in a single motion, from the existing vial to a sterile viewing chamber. Be sure to keep the endothelial side up. Place the cap on the chamber. Keep chambers containing tissue and media on sterile field. Remove vial(s) from LFH. Remove and discard sterile gloves.
- Spike balanced salt solution (BSS) bottle with infusion line. Hang bottle of sterile BSS approximately four feet from working area surface.
- Open two pairs of sterile gloves and sterile gown with towel.
- Perform six minute surgical scrub and dry hands.
- Put on sterile gown, then both pairs of sterile gloves.
- Open instrument boxes and place the contents onto the sterile field.
- Dispense 10-20 cc of BSS solution into metal basin or medicine cup. Fill sterile pipette with BSS solution. Connect stopcock and infusion line to infusion port of the anterior chamber and flush with BSS so that a small amount is visible on top of the piston.
- Position artificial chamber in LFH on top of gauze. Lower piston by turning graft tightening ring counterclockwise.
2. Procedure
- Using forceps, gently grasp cornea by scleral rim. Open stopcock to flush system with BSS while carefully centering cornea on top of the piston with the endothelial side down. If bubbles are visible beneath the cornea, continue infusing with BSS and slightly moving the cornea to remove them. Discontinue infusion once air bubbles are removed. Ensure that the cornea is centered on the piston (Figure 3a).
- Position anterior chamber cover on base locking ring so that the tabs of the cover fit into the open spaces on the base. Lock cover into base by turning cover clockwise 15°. Raise piston up and tighten completely (Figure 3b).
- With a sterile gloved finger, touch top of cornea to ensure that there is sufficient pressure to perform procedure.
- Check pachymetry by placing probe on surface of cornea to obtain thickness reading (Figure 4). The standard deviation must be less than 10. If not, retake measurement. With the sterile gloved hand that was not used to perform the pachymetry, pass the turbine hose to the hand that performed pachymetry and screw the turbine hose into the control unit. Have the assisting technician record pachymetry reading.
- Remove contaminated gloves.
- Using sterile marking pen, draw a 4mm line from limbus toward center of the cornea (or do not mark if surgeon prefers no marking). Use pipette to place five drops of BSS on top of the cornea.
- Unless specific instructions are provided by the surgeon, the 300 μm cutting head will be used if the pre-cut pachymetry measurement is less than 600 μm. If over 600 μm, the 350 μm cutting head will be used.
- With thread facing toward you and number facing up, load blade into right side of microkeratome head, pointed end first, avoiding contact with the blade.
- Holding head at each side, screw head onto turbine. Tighten the artificial chamber with fingers.
- Screw turbine onto turbine hose.
- Test the blade oscillation by pressing the vacuum pedal once, submerging the cutting head in the sterile water and pulse the turbine for 5 seconds.
- Retighten piston.
- Place microkeratome onto the base with mounting post and position at five o’clock. Press and hold turbine pedal to oscillate blade (Figure 5a).
- Using index finger and thumb, hold microkeratome midway between the base and the top of the turbine. Turn wrist to make a smooth, even cut through and across the cornea. Release turbine pedal and lift microkeratome straight off unit. Press vacuum pedal to turn off vacuum (Figure 5b).
- Don a sterile glove and recheck pachymetry reading after corneal cap is removed by placing probe on corneal surface to obtain second thickness reading being mindful that the tissue is very thin and easily damaged. Remove contaminated glove. Have assisting technician record second pachymetry reading.
- Using sterile marking pen, place a mark if requested by surgeon, on the mid-peripheral edge of the residual stromal bed in the artificial chamber. Place a few drops of sterile BSS onto residual stromal bed.
- Remove the anterior cornea cap from the microkeratome (Figure 6) and replace it onto the cornea before removing cornea from artificial anterior chamber. Cap should be centered on cornea using peripheral marking to align the cap correctly if applicable. Use swab spear to gently reposition the cap onto the cornea. Use fresh spear to absorb any BSS underneath anterior cap.
- Open stopcock, turn chamber upside-down and lower piston slow enough to prevent cornea from deforming. Unlock base and allow pressure from the BSS flow to push the artificial chamber cup from the base. With forceps, gently pull at the corneal rim at 9, 12 and 3 o’clock positions to loosen it from the cup. Once loosened, use forceps at the 12 o’clock position to remove cornea. Place the cornea in the viewing chamber, endothelial side up (Figure 7). Place the lid on the viewing chamber. Remove sterile glove.
- Tighten viewing chamber lid.
- Perform post-cut slit lamp evaluation and specular microscopy of cornea and record findings.
- Place chamber(s) in appropriate section of refrigerator.
- Package for transport to surgeon (Figure 8).
3. Representative Results
Proper mechanical microkeratome dissection of the donor cornea results in smooth, uniform lamellar corneal donor tissue. This is shown by an optical coherence tomography (OCT) image of the cornea in cross section (Figure 9). The final posterior corneal tissue should be of adequate thickness as measured by pachymetry. Over the past 6 months at the Michigan Eye Bank, the mean pre-processing corneal thickness was 558 microns, and post-processing thickness of the posterior corneal tissue was 158 microns. Eighty-seven percent of microkeratome-dissected donor tissue measured between 100-200 microns, 10.9% measured >200 microns, and 2.1% measured <100 microns.
The posterior corneal tissue must retain high endothelial cell density (ECD) to provide improved endothelial function to the transplant recipient. Specular microscopy is used to measure ECD. In the past 6 months, all of the corneal tissue deemed eligible for endothelial keratoplasty from the Michigan Eye Bank had an ECD of >2200 cells/mm2. Ninety-nine percent of the precut DSAEK tissue had a post-processing ECD >2400 cells/mm2, and 19% had an ECD > 3000 cells/mm2. The mean change in pre- to post-processing ECD was negligible at 1.2% (p=0.0003, paired two-tailed t-test). Complications that can occur during the procedure include loss of pressure, asymmetric dissection, and significant tissue indentation (resulting in corneal endothelial cell loss). Improper dissection can also result in tissue perforation.
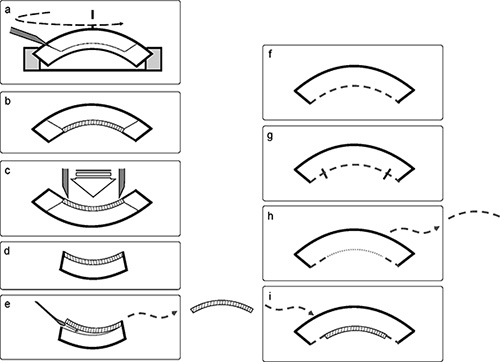
Figure 1. Overall Scheme of Corneal Tissue Preparation for Endothelial Keratoplasty Figures 1a to 1e are cross-section representations of the donor cornea preparation. Figures 1f to 1i are cross-section representations of the transplant recipient’s cornea during DSAEK surgery.
- The donor cornea is mounted onto an artificial anterior chamber and dissected with the microkeratome head.
- After tissue dissection, the two lamellae are separate but the anterior lamella (cap) is positioned back onto the remained corneal bed for transportation to the surgeon.
- In the operating room, the surgeon uses a trephine to cut the central corneal tissue vertically through both anterior and posterior lamella.
- After trephine cutting, the peripheral donor cornea is removed from the field.
- The posterior lamella is gently removed from the anterior lamella with a spatula. The donor posterior lamella (DSAEK tissue) replaces the diseased portion of the recipient cornea (1i).
- The patient has a diseased posterior cornea to be removed.
- The diseased posterior cornea is scored with an intraocular instrument (reverse Sinsky hook) in a large diameter circle.
- After scoring the diseased cornea, the posterior corneal membrane is removed.
- The donor posterior lamella (DSAEK tissue) is placed in the recipient’s eye.
Figure 2. Corneal Tissue in Media. Corneal tissue is in preservation media after harvesting from donor.
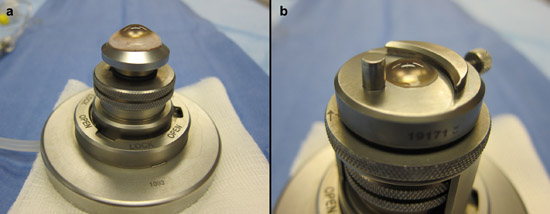
Figure 3. Corneal Tissue on Artificial Anterior Chamber.
- Corneal tissue is mounted onto the artificial anterior chamber prior base locking ring or tissue dissection.
- Corneal tissue is mounted onto artificial anterior chamber with base locking ring sealed over the tissue.
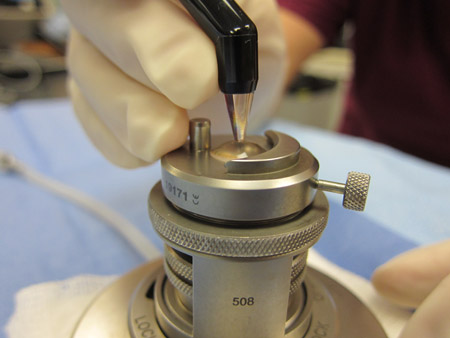
Figure 4. Corneal Tissue Thickness Check. The corneal thickness is checked using ultrasound pachymetry probe on surface of cornea.
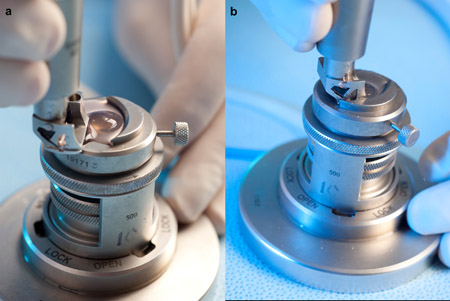
Figure 5. Corneal Tissue Dissection.
- Microkeratome blade is placed on the base with mounting post and position at five o’clock.
- Microkeratome is passed through cornea to make the lamellar dissection.

Figure 6. Anterior Cap of Cornea after Dissection. The anterior cornea cap is free after microkeratome dissection is complete.

Figure 7. Dissected Cornea in Viewing Chamber. After dissection is completed, the cornea is returned to the viewing chamber for transportation.

Figure 8. Cornea in Packaging for Transportation. The cornea in the viewing chamber is then securely packaged for transportation to the surgeon.
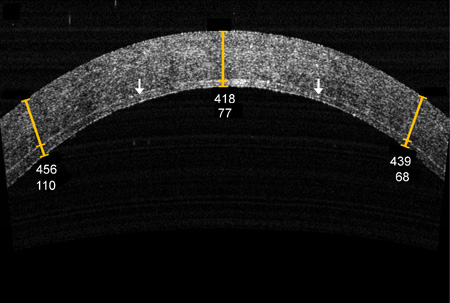
Figure 9. OCT Appearance of Cornea. The OCT of the final dissected cornea (in cross-section) shows that the cornea is split into two halves. The interface is more intensely reflective than the surrounding tissue as indicated by the arrow.
