Figure 5 shows the proof-of-principle experiments using Evan’s blue dye, allowing us to test the system and visualize appropriate fluid and placental barrier function and to prevent containment transfer to the fetal compartment. The Evan’s blue dye reached and perfused the tissue of the placenta within this system (Figure 5A). Upon further investigation, it is clear that the Evan’s blue dye did not enter the fetal umbilical vein (Figure 5B), which is expected as Evan’s blue dye is bound to albumin.
Figure 6 shows data for the mock experiment described in this protocol. Effluent samples from the distal end of the uterine artery and fetal umbilical vein were measured at each 10-minute segment to evaluate the fluid flow over time after the bolus dose was administered to the maternal uterine artery (Figure 6). Reduced fluid transfer to the fetal compartment within 10 minutes after polystyrene infusion was identified. To quantify the transfer of polystyrene to the fetal compartment during the time course when it occurs, 25 µL of the perfused fluid from each time point was placed in a 96 well plate in duplicate to measure the sample fluorescence. Fluorescence was determined by spectroscopic reading at 546/575 nm (ex/em) using a fluorescent microplate reader. Polystyrene transfer to the fetal compartment occurred within 10 minutes and peaked at 20 minutes and continued for 90 minutes (Figure 6B).
A subset of perfused placental tissues were saved for histopathology and morphological assessments. The tissues were formalin-fixed and hematoxylin and eosin stained and reviewed by a board certified veterinary pathologist. These experts identified no structural abnormalities in placentas perfused by only PSS, or PSS with the bolus dose of rhodamine-labeled polystyrene.
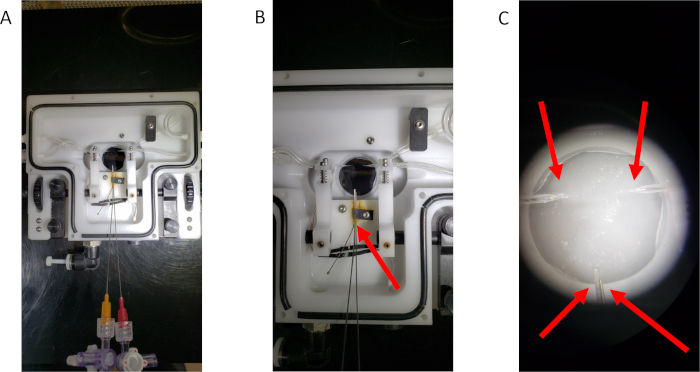
Figure 1: The modified single vessel chamber. (A) An overview of the modified chamber. (B) A close-up image of the blunt-tip needles secured within the vessel chamber. The red arrow indicates the thermistor clip that has been altered to hold the needles in place for umbilical cannulation. (C) A representative image of the four cannulas prepared for tissue cannulation. Red arrows point to each of the four cannulas. Please click here to view a larger version of this figure.
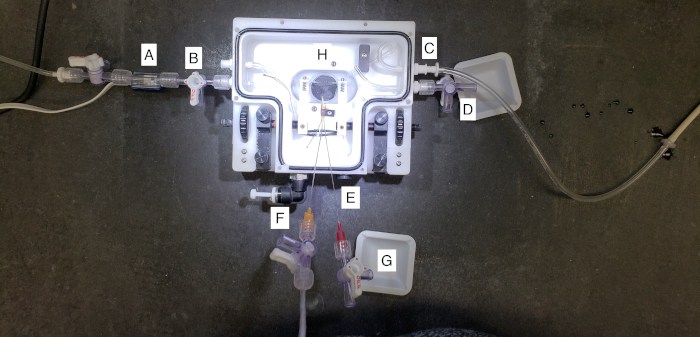
Figure 2: A closer view of the placental perfusion chamber. (A) This represents the tubing attached to the pressure transducer and cannulated the proximal maternal uterine artery, or the “inflow”. Pressure is set to a constant 80 mmHg as defined by the literature. (B) This represents the chamber drain port of the superfusate surrounding the placental tissue during perfusion. (C) This represents the chamber inflow of the superfusate to bathe the placenta with warmed PSS during perfusion. (D) This represents the distal maternal uterine port where effluent from the uterine perfusion may be collected. (E) This represents the temperature port, where the vessel chamber can be attached to a thermometer and heater to maintain a consistent temperature throughout the experiment. (F) This represents the umbilical artery cannulation. The umbilical artery is pressurized to 50 mmHg to allow for countercurrent flow at the level of the placenta. (G) This represents the umbilical vein effluent collection. Fluid that flows toward the fetal compartment during perfusion will be collected here. (H) This is the center of the perfusion system, where the placenta is cannulated and maintained throughout perfusion. Please click here to view a larger version of this figure.
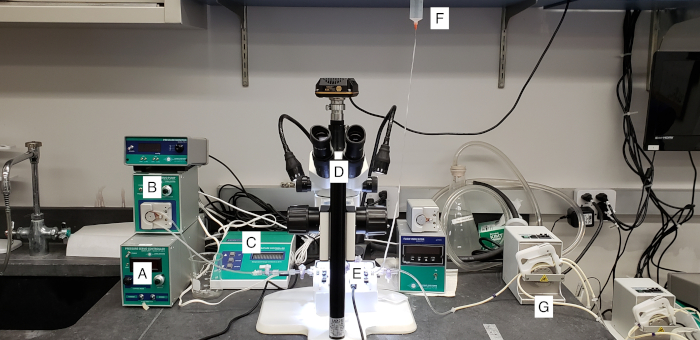
Figure 3: A view of the placental perfusion system. (A and B) The pressure control system used to monitor and maintain 80 mmHg of perfusate through uterine artery. (C) This represents the thermo-regulation of the perfusion chamber. (D) Microscope. (E) Perfusion chamber. (F) Gravity-fed umbilical artery perfusion set at 50 mmHg. (G) A peristaltic pump used to fill and drain placental superfusate PSS. Please click here to view a larger version of this figure.
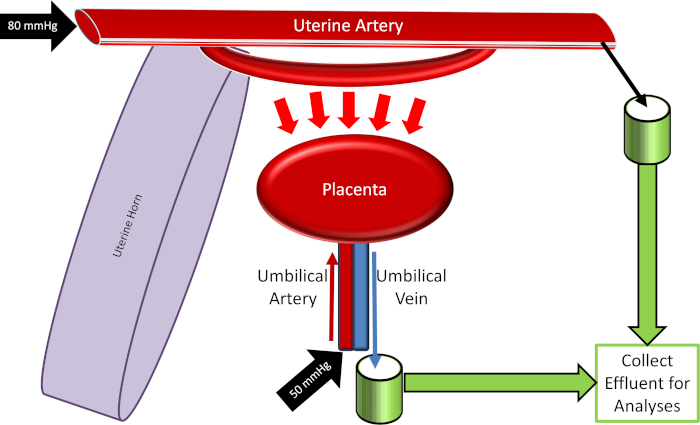
Figure 4: Schematic of the placental perfusion system. Please click here to view a larger version of this figure.
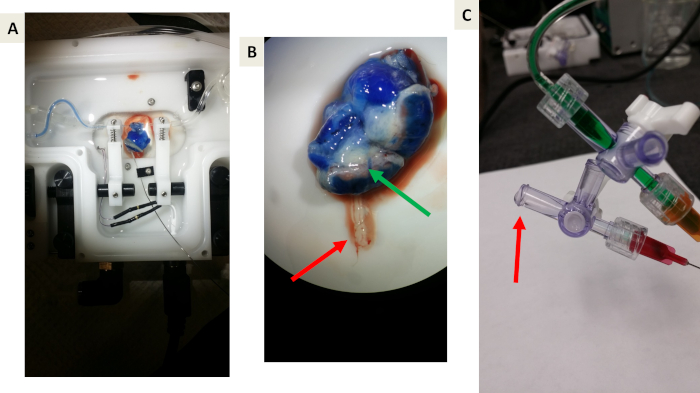
Figure 5: Representative images of proof-of-principle experiments using Evan’s blue dye. (A and B) Proof-of-principle that Evan’s blue will perfuse the uterine vasculature, uterine muscle, and placenta but will not cross the placental barrier due to albumin binding. The green arrow indicates the blue venous drainage from the placenta back to the maternal circulation. The Red arrow indicates the umbilical vein effluent toward the fetal compartment. Note the lack of blue dye. (C) A representative image of collecting effluent draining from the umbilical vein. The red arrow indicates drop formation prior to collection. Please click here to view a larger version of this figure.
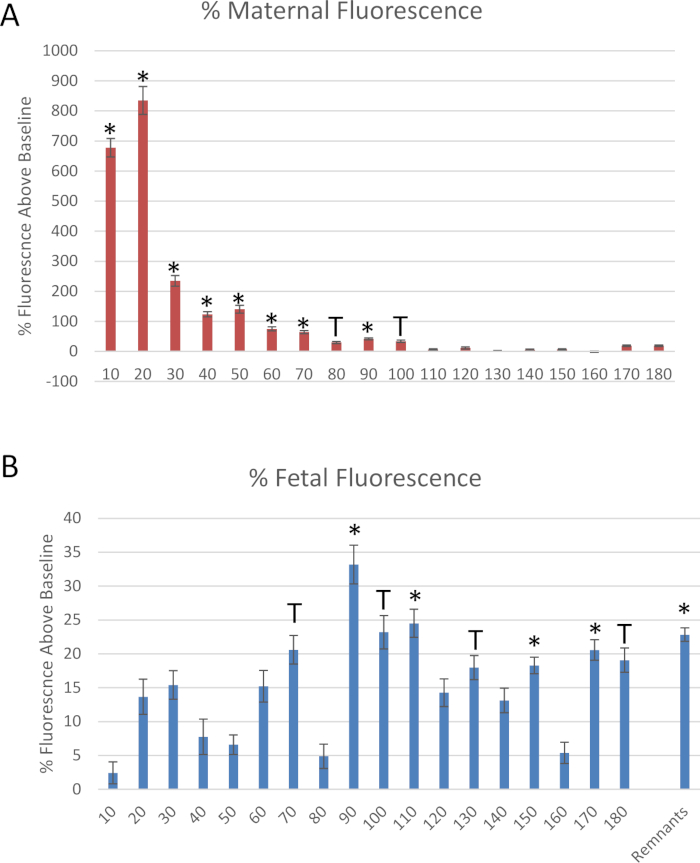
Figure 6: Data derived from the mock experiment. Fluorescence measurements of rhodamine-labeled polystyrene nanomaterials, normalized to baseline fluorescence, through the collection of (A) uterine artery and (B) fetal umbilical vein effluents. Mean normalized to baseline fluorescence ± standard error (SE). *: p < 0.05 and T: p < 0.1 via analysis of variance (ANOVA). Please click here to view a larger version of this figure.
