Figure 6 represents a scheme of all the outcomes of a biopsy procedure that can be adopted to standardize the protocol and monitor the performance of each operator. The main procedural outcome is the timing to complete the biopsy/biopsies; the main technical outcome is the quality of the plot produced after genetic testing that might result in either a conclusive or inconclusive diagnosis, the latter of which requires a re-biopsy of the undiagnosed blastocyst; the main biological outcome is the rate of cryo-survival and re-expansion versus degeneration after warming; lastly, the main clinical outcome is the live birth rate after vitrified-warmed blastocyst transfer. In three previous studies we reported the KPIs defined at the center(s) for the technical, biological and clinical outcomes11,13,16. Hereafter, we instead report how the KPI for the timing of biopsy was defined. Moreover, the putative influence of the timing between biopsy and vitrification on the post-warming behavior of euploid blastocysts was also investigated.
In a 2 year period, a total of 1,544 trophectoderm biopsy procedures were conducted by 7 operators (Table 1). All biopsied blastocysts were then moved back to the incubator into a post-biopsy culture dish until vitrification. All the relevant data were collected in a relational database. All the timings of biopsy and between biopsy and vitrification were retrospectively obtained from the software of the IVF electronic witnessing system. The data were then exported and analyzed for statistics.
The cryo-survival rate of euploid blastocysts after trophectoderm biopsy and vitrification-warming was N = 571/572, 99.8%. The re-expansion rate at 1.5 h after warming was N = 556/571, 97.4%. Among the 15 not re-expanded blastocysts, one resulted in a live birth after being transferred in utero. The live birth rate after vitrified-warmed euploid single blastocyst transfer was N=227/572, 39.7%.
Definition of the ideal timing of biopsy
Table 1 summarizes the relevant data of the biopsy procedures conducted. Overall, 1.89 ± 1.03 (range 1-4) blastocysts were biopsied per procedure in 8.24 ± 4.23 min (range 3-22). The mean timing of biopsy varied because of both the number of blastocysts biopsied per procedure, from a minimum of 5.78 ± 2.94 min (range 3-16) when only one embryo was laid in the dish to a maximum of 12.93 ± 4.43 min (range 6-22) when the embryos sequentially biopsied were 4. Another relevant parameter was the operator involved in the procedure: the most expert (N = 443 procedures) was the fastest (7.41 ± 3.6 min, range 3-22), while the least experienced (N = 42) was the slowest (14.19 ± 4.24 min, range 6-22). Indeed, a generalized linear model entailing both the “number of blastocysts biopsied per procedure” and the “operator” variables perfectly explains the “timing of biopsy” with a R2 = 0.48 and a power = 1. This analysis was useful to define that ideally ~6 min is enough for a blastocyst biopsy procedure when only an embryo is laid in the dish, while ~9 min, ~12 min and ~13 min for 2, 3 and 4 blastocysts, respectively. Clearly, the whole procedure entails also moving the embryos from the culture to the biopsy dish and from the latter to the post-biopsy culture dish after the procedure, as well as changing the biopsy pipette between sequential biopsies.
Figure 7 plots the mean timing of biopsy for each operator along the study trimesters (from the 1st to the 8th). The dotted red line identifies the mean overall value of 8.24 min. Such a graph is useful to monitor the mean performance of each practitioner. For instance, the most expert operators (1 and 2) showed a constant decrease of this timing, which suggests a trend typical of a learning curve. All the operators from 3 to 6 were instead sufficiently constant in their performance around the mean overall value across the trimesters. Anytime they showed a peak in the mean value from a given trimester (e.g., operator 3 in the 7th trimester, operator 4 in 6th trimester, operator 5 in the 3rd trimester), they were warned in order to revise their performance. Operator 7 (i.e., the least experienced) showed timings typical of an embryologist that has just finished his/her training. Possibly, he/she will meet the standards internal to the lab as the expertise would increase.
Importantly, the time of biopsy was similar across re-expanded and not re-expanded euploid blastocysts at 1.5 h from warming (9.52 ± 4.23 min, range 3-22 versus 10.5 ± 5.68 min, range 4-22; t-test = 0.37). Likely, implanted (N = 229) and not implanted (N = 343) vitrified-warmed euploid blastocysts also showed comparable biopsy timings (9.77 ± 4.15 min, range 3-22 versus 9.41 ± 4.36 min, range 3-22; t-test = 0.39). Possibly then, a timing ≤22 min to biopsy up to 4 blastocysts does not affect embryo behavior after warming. Therefore, we defined this value as maximum threshold.
Similarly, no difference was shown in terms of live birth rate across the different biopsy operators, as already reported previously13 (Supplementary Table 1).
Another important parameter to monitor each operator’s performance is the rate of inconclusive results after diagnosis, which should be as close as possible to the general performance of each laboratory. Ideally this rate should not exceed 2.5% and might decrease with time due to an increasing expertise in biopsy and tubing procedures16. The target number of TE cells to retrieve are 7-8 according to two previous studies13,16. To this end, it is suggested to take a picture of the biopsied fragment for quality control purpose (see some examples in Figure 3). Such picture might be checked in case of inconclusive diagnoses to evaluate whether the cause was imputable to the dimension/quality of the fragment (i.e., low quality of the molecular analysis), to the tubing (i.e., DNA amplification failure) or to some issues in the processing of the sample in the genetic laboratory.
Definition of the ideal timing between biopsy and vitrification
In the study period, 572 euploid blastocysts were warmed to undergo an embryo transfer after a diagnosis of euploidy. Figure 8A shows each warmed blastocyst as a black circle distributed across the increasing timing between biopsy and vitrification and clustered in two groups according to the outcome under investigation: re-expanded or not re-expanded within 1.5 h from warming. All the blastocysts (N = 117/117) vitrified within 30 min, 97.6% (N = 245/251) of the blastocysts vitrified between 31-90 min, and 95.1% (N = 194/204) of the blastocysts vitrified beyond 90 min re-expanded, respectively (no re-expansion rates: 0%, 2.4% and 4.9%). Therefore, we set 30 min and 90 min as the early and late thresholds of time between biopsy and vitrification.
Figure 8B shows the re-expansion rate in the three groups (≤30 min, 31-90 min, >90 min) further sub-clustered according to the blastocyst quality and day of preimplantation development. Especially for poor quality and/or day 7 blastocysts, the timing between biopsy and vitrification seems crucial to achieve re-expansion after warming. Specifically, the odds-ratio of re-expansion after warming corrected for both blastocyst quality and day of biopsy in blastocysts vitrified within 30 min from biopsy versus blastocysts vitrified beyond 90 min was 3.05 (95% CI 1.01-9.4, p=0.05). Instead, the period in between these two thresholds (31-90 min) represented a grey area that might or might not have an impact.
Only 1 out of 15 not re-expanded blastocysts resulted in a live birth after transfer. Therefore, we lastly investigated the live birth rate achieved after warmed euploid single blastocyst transfer clustered in the three groups according to the timing between biopsy and vitrification. The highest live birth rate was achieved by transferring euploid blastocysts vitrified ≤30 min from the trophectoderm biopsy (N = 56/117, 47.9%). However, this result did not reach statistical significance when compared to the same outcome obtained either with blastocysts vitrified between 31 and 90 min (N = 92/251, 36.7%; Fisher’s exact test = 0.06), or with blastocysts vitrified >90 min from the biopsy (N=81/204, 39.7%; Fisher’s exact test = 0.16). Therefore, either a negative effect on blastocyst reproductive competence is negligible or the sample size in this dataset (N = 572) was insufficient to reach statistical significance.
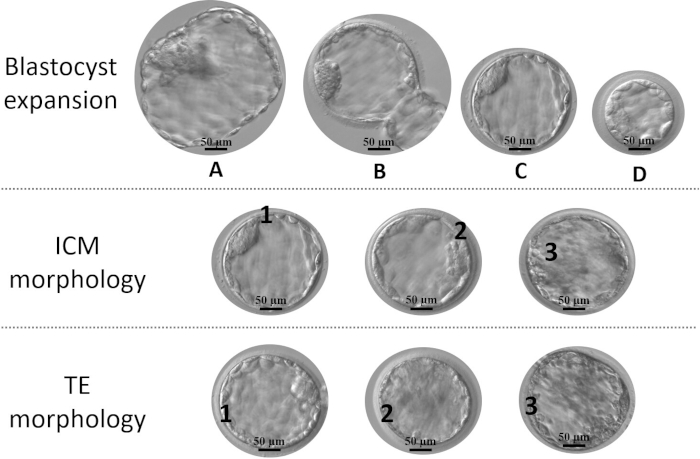
Figure 1: Parameters for blastocyst grading. Expansion: (A) fully hatched, (B) in hatching, (C) fully expanded, and (D) not expanded. The ideal stage is C, while a blastocyst D should be given more time to achieve full expansion, unless this stage is reached in day 7; Inner cell mass (ICM) morphological quality: 1 (noticeable with several strictly packed cells), 2 (discernable with several but roughly packed cells) and 3 (difficult to distinguish with very few low-quality cells); trophectoderm (TE) morphological quality: 1 (well-organized epithelium with several cells), 2 (loose epithelium with few cells) and 3 (few and/or large low-quality cells). Please click here to view a larger version of this figure.
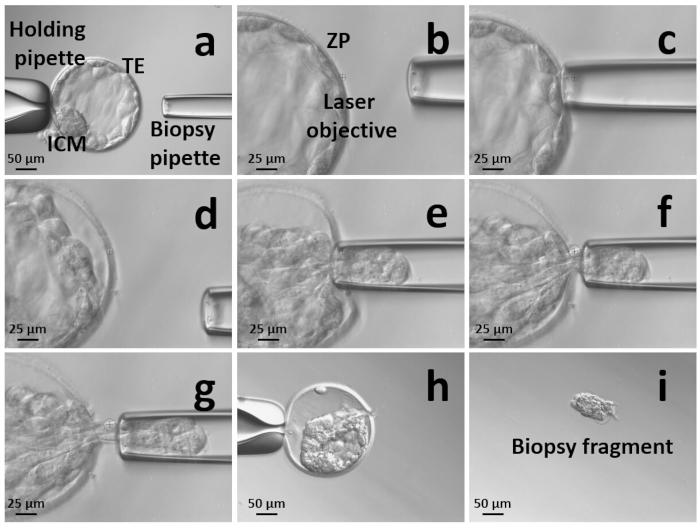
Figure 2: Summary of the sequential zona pellucida (ZP) opening and trophectoderm (TE) cells retrieval approach for blastocyst biopsy. (a) Orient the blastocyst with the inner cell mass (ICM) close to the holding pipette and far from the spot where the selected TE cells will be retrieved. Secure the blastocyst on the holding pipette; (b) open the ZP through 2-3 laser shots; (c) blow some culture media through the hole; (d) the blastocyst will detach from the ZP; (e) enter the ZP and suck 5-10 TE cells in the biopsy pipette; (f) move backwards with the biopsy pipette to stretch the selected fragment and expose the junctions between the cells; (g) fire at the junctions between the cells and continue stretching the fragment until the TE cells are released from the body of the blastocyst; (h) the blastocyst after TE biopsy is collapsed; (i) take a picture of the biopsy fragment for quality control and transfer it to the PCR tube that will be sent to the genetic laboratory. Please click here to view a larger version of this figure.
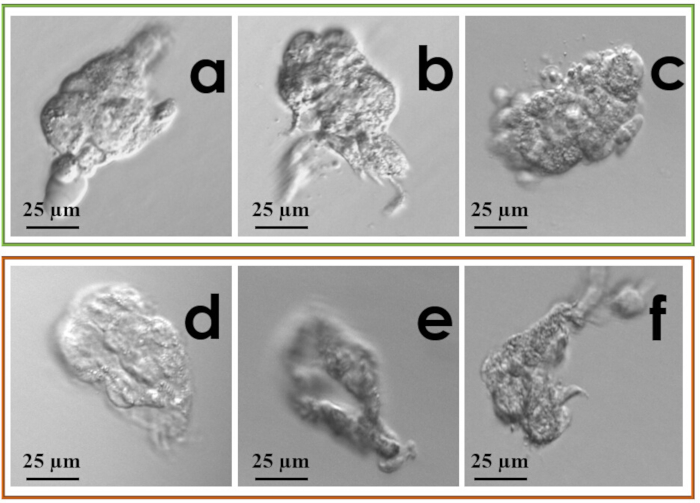
Figure 3: Examples of biopsy fragments: (a-c) desirable fragments; (d) lysed fragment; (e) small fragment with degenerated cells; (f) small, partially lysed and degenerated fragment. Please click here to view a larger version of this figure.
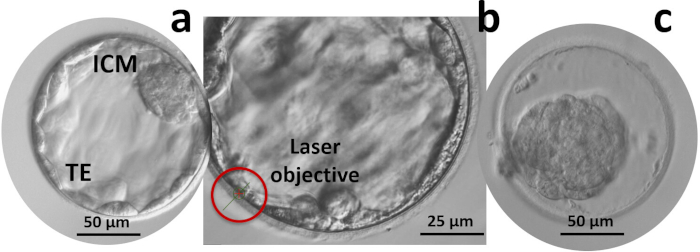
Figure 4: Artificial shrinkage. (a) Orientate the blastocyst so that the inner cell mass (ICM) is far from the targeted section of the trophectoderm (TE); (b) Fire 2-3 laser shots in a row at the junctions between TE cells and moving outwards; (c) Wait for the blastocyst to collapse before starting vitrification. Please click here to view a larger version of this figure.
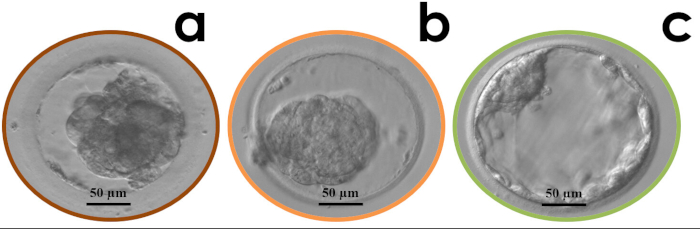
Figure 5: Examples of blastocyst degeneration (a), cryo-survival but no re-expansion (b) and cryo-survival and full re-expansion (c) 1.5 h post-warming. Please click here to view a larger version of this figure.
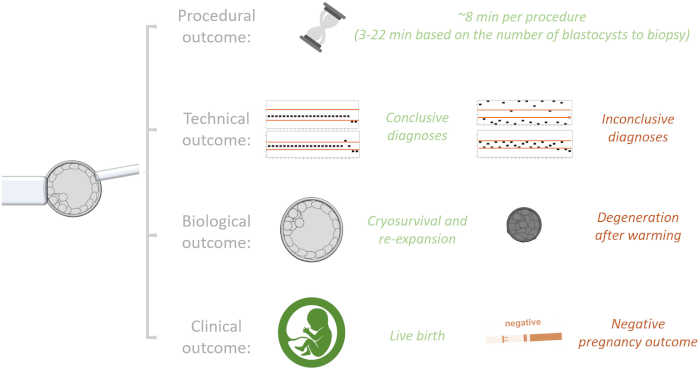
Figure 6: Summary of the different outcomes of trophectoderm biopsy that might be used to monitor the performance of an operator and define the key performance indicators internal to each laboratory. The main procedural outcome is the timing of biopsy. The main technical outcome is the rate of conclusive (euploid or aneuploid) and inconclusive diagnoses (re-biopsy required) obtained; the latter might be caused by DNA amplification or low-quality molecular data, both resulting in not-interpretable chromosome copy number profile plots. The main biological outcome is the rate of cryo-survival and re-expansion or degeneration after biopsy, vitrification and warming. The main clinical outcome is the rate of live births or negative pregnancy outcomes achieved after vitrified-warmed blastocyst transfer. Of note, while the procedural outcome is exclusively dependent on the operator and the number of blastocysts to biopsy per procedure, all other outcomes might be affected from other confounders independent from the biopsy operator (e.g., the steps and operators involved in the molecular analysis, the morphological quality of the blastocyst, the day of biopsy) that should be accounted to properly evaluate his/her performance. Please click here to view a larger version of this figure.
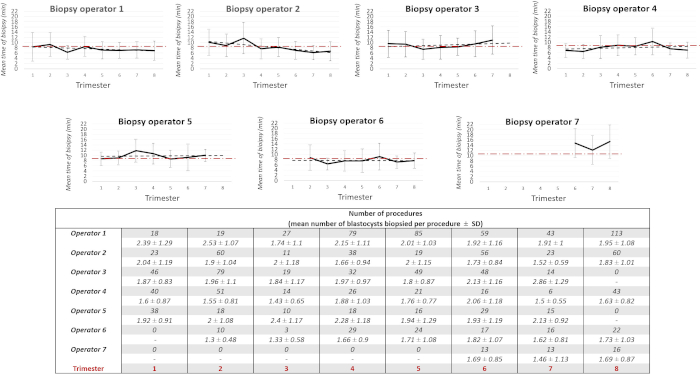
Figure 7: Mean timing of biopsy per operator across the 8 study trimesters. The table summarizes the related number of procedures and the mean number of blastocysts biopsied per procedure by each operator in the 8 study trimesters. The dotted red line within each graph represents the overall mean timing of biopsy (8.24 min). The error bars are the standard deviations. Please click here to view a larger version of this figure.
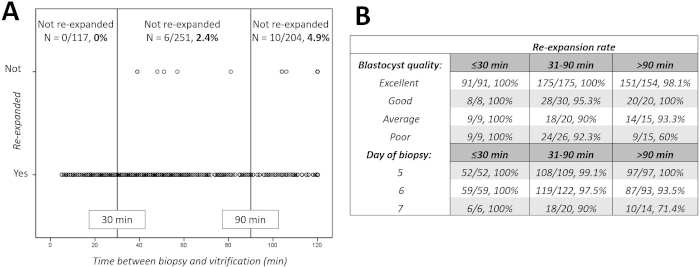
Figure 8: Re-expansion after warming versus timing between biopsy and vitrification. (A) shows not re-expanded and re-expanded blastocysts 1.5 hr after warming. Each blastocyst is represented by a black circle across the increasing timings. The vertical continuous black lines represent 30 min set as early threshold and 90 min set as late threshold. (B) shows the re-expansion rates in the three groups (timing between biopsy and vitrification: ≤30 min, 31-90 min, >90 min) further clustered according to blastocyst quality and day of biopsy. Please click here to view a larger version of this figure.
| N of procedures | N blastocysts biopsied per procedure | Mean timing of biopsy ± SD, range (min) | |
| Operator 1 | 443 | 2.01 ± 1.09, 1-4 | 7.41 ± 3.6, 3-22 |
| 195 | 1 | 4.75 ± 1.96, 3-16 | |
| 111 | 2 | 7.83 ± 2.45, 3-18 | |
| 71 | 3 | 10.27 ± 2.41, 4-16 | |
| 66 | 4 | 11.48 ± 3.81, 6-22 | |
| Operator 2 | 290 | 1.81 ± 0.98, 1-4 | 7.87 ± 4.13, 3-22 |
| 142 | 1 | 5.69 ± 3.32, 3-16 | |
| 89 | 2 | 8.48 ± 2.79, 3-18 | |
| 30 | 3 | 11.37 ± 3.72, 4-20 | |
| 29 | 4 | 13.1 ± 3.89, 9-22 | |
| Operator 3 | 287 | 1.98 ± 1.05, 1-4 | 9.10 ± 4.65, 3-22 |
| 121 | 1 | 6 ± 2.19, 3-15 | |
| 89 | 2 | 9.6 ± 3.87, 3-22 | |
| 38 | 3 | 12.66 ± 4.55, 4-22 | |
| 39 | 4 | 14.13 ± 4.8, 6-22 | |
| Operator 4 | 217 | 1.66 ± 0.87, 1-4 | 7.58 ± 3.45, 3-22 |
| 118 | 1 | 5.58 ± 1.96, 3-14 | |
| 66 | 2 | 8.92 ± 2.91, 4-22 | |
| 21 | 3 | 11.48 ± 2.34, 5-16 | |
| 12 | 4 | 13 ± 4.26, 6-19 | |
| Operator 5 | 144 | 2.03 ± 1.08, 1-4 | 9.43 ± 4.24, 3-22 |
| 59 | 1 | 6.15 ± 2.5, 3-16 | |
| 43 | 2 | 10.07 ± 2.73, 6-16 | |
| 20 | 3 | 12.6 ± 2.89, 9-18 | |
| 22 | 4 | 14.09 ± 4.43, 6-22 | |
| Operator 6 | 121 | 1.67 ± 0.94, 1-4 | 7.79 ± 3.93, 3-22 |
| 70 | 1 | 6.19 ± 2.95, 3-16 | |
| 32 | 2 | 8.12 ± 1.72, 3-11 | |
| 9 | 3 | 12.78 ± 3.31, 9-18 | |
| 10 | 4 | 13.5 ± 6.19, 6-22 | |
| Operator 7 | 42 | 1.62 ± 0.94, 1-4 | 14.19 ± 4.24, 6-22 |
| 27 | 1 | 11.85 ± 5.53, 6-16 | |
| 6 | 2 | 16.5 ± 3.73, 11-22 | |
| 7 | 3 | 19.86 ± 3.34, 13-22 | |
| 2 | 4 | 19 ± 4.24, 16-22 | |
| Total | 1544 | 1.89 ± 1.03, 1-4 | 8.24 ± 4.23, 3-22 |
| 732 | 1 | 5.78 ± 2.94, 3-16 | |
| 436 | 2 | 8.85 ± 3.14, 3-22 | |
| 196 | 3 | 11.72 ± 3.70, 4-22 | |
| 180 | 4 | 12.93 ± 4.43, 6-22 |
Table 1: Total mean timing of biopsy and mean number of blastocysts biopsied in each procedure according to biopsy operator. The mean timing of biopsy has been also shown according to each sequential number of blastocysts biopsied per procedure. A generalized linear model that includes both the “biopsy operator” and “number of blastocysts biopsied per procedure” variables perfectly correlates with the “timing of biopsy” (R2 = 0.48, power = 1).
Supplementary Figure 1: Main devices and supports required for the procedure. Please click here to download this file.
Supplementary Table 1: Logistic regression analysis does not show any significant association between the biopsy operator and live birth after vitrified-warmed euploid blastocyst transfer. Please click here to download this file.
