General remarks:
All operations should be performed under an upright dissecting microscope (Olympus, SZX10 with Z-Axis Crank Post with STU2 Stand Boom Stand) and by using a surgical coagulator (11). The experimental groups should be matched as best as possible in age and weight to ensure comparability of the results. Temperature, blood pressure, anesthesia and fluid administration should be stable throughout.
1. Anesthesia and trachea preparation
- Use C57BL/6 mice that are at least 10 weeks old and have a body of 22-25 g. Induce Anesthesia using sodium pentobarbital at a dose 70 mg/kg body weight i.p (6). Maintain anesthesia approximately with 10 mg/kg/h sodium pentobarbital. Be cautious with overdosing since this might significantly lower the blood pressure. Re-dosing of pentobarbital – even after hrs- can lead to severe increases in plasma levels.
- After anesthesia induction, secure mice in a supine position with the upper and lower extremities attached to the table using a tape and a suture fastened to the ankles. Do the same for the head by using the teeth. Sufficient restraining is important for a successful intubation and a well controlled surgery. Prior to surgery, cover the mouse with mineral oil to reduce the risk of mouse hair allergy. In order to ensure that the body temperature remains stable cover the mice with commercially available food wrap.
- Place mice on a temperature-controlled heated table (RT, Effenberg, Munich, Germany) with a rectal thermometer probe attached to thermal feedback controller to maintain body temperature at 37°C.
- Expose the trachea surgically. Dissect lateral and dorsal sides of the trachea of the connective tissue and place two 3.0 silk surgical suture (Harvard apparatus, USA) each 10 cm long underneath the trachea. The sutures should be approximately 1 cm apart.
- Carefully incise the trachea 3 – 4 mm below larynx between two circular cartilages using a McPherson-Vannas Scissors (8 cm, straight blade; World Precision Instruments, USA). Make sure not to cause a bleeding, since this might confound the outcome parameters.
- Perform a tracheal intubation using a blunt polyethylene cannulae (Insyte 22g, Beckton Dickinson, USA). Insert the tip of the polyethylene cannulae in an 85 degree angle into the trachea. Then tilt the cannulae so it is in line with the tracheal lumen. Slowly advance the tube further down the trachea until the tip of cannulae has disappeared in the thorax aperture. Fixate the tube in this position with the two surgical silk suture placed dorsal of the trachea (see 1.4).
2. Technique of ventilator-induced lung injury
- Connect the tube to a ventilator. To induce lung injury we use a pressure controlled ventilation technique by using a Servo 900 C from Siemens (DRE Veterinary, USA). Animals will be ventilated using peak inspiratory pressure of 45 mbar, frequency of 80 breaths/min and a positive end-expiratory pressure of 0-3 mbar with a FiO2 = 1.0. The inspiration to expiration ratio should be 1:1. Despite of the fact that the Servo 900 C is built as ventilator for humans, its use in a pressure controlled ventilator setting works excellent for the ventilation of mice.
- Monitor heart rate with an ECG (e.g. Hewlett Packard, B blingen, Germany). Make sure that the heart rate does not drop below 400. One should see a shift of the heart axis to the right, when mechanical ventilation is instituted as a sign of increased pulmonary artery pressures subsequent to an increase in intrathoracic pressure. If the mouse develops bradycardia, check the temperature and the anesthetic dose/concentration. Xylacin/ Ketamin anesthesia induces a heart heart of 250/ min and is therefore not recommended.
- Apply a proper fluid replacement. An infusion with normal saline 0.1 ml/hour via an arterial or venous catheter should be performed prior to the ventilation to ensure sufficient venous filing. Due to the high ventilation pressures the venous return to the heart is impaired, which might lead to a critical drop of the mean arterial pressure. Also, a saline bolus of 500 μl could be given i.p. prior to surgery.
- Place a catheter in the carotid artery for continuous recording of blood pressure (27). Attach the arm to the body before you start dissecting the artery. The carotid artery is exposed via blunt dissection of the paratracheal muscles. Following further exposure and careful avoidance of any tissue trauma (particular of the vagal nerve), a catheter is inserted into the vessel using two sutures and a small clamp (37). This will expose a longer segment of the artery. Place a ligature at the very end of the carotid artery. Attach a larger clamp to the end of the suture to obtain tension or fixate the suture to the table using tape. Place another suture around the artery and dissect the artery to the very distal end. Here, place a small clamp. Use micro scissors to cut a small diagonal opening into the artery. Hold the opening with a fine forceps (Dumont, WPI) and advance the proper sized catheter with your hands/forceps. Make a knot with your second suture and secure the artery. Loosen the clamp and advance the catheter further. Secure the catheter with several knots and tape. Alternatively the carotid artery catheter can be place at the end of the experiment to collect arterial blood samples for blood gas analysis.
3. Recovery of tissue samples
After 3 hours of mechanical ventilation, samples are collected to assess the extent of lung injury. We recommend collecting brochnoalveolar lavage fluid (BAL), arterial blood and lung tissue.
- Obtain BAL fluid at the end of the experiment. After deepening of anesthesia, flush the tracheal tube with 1 ml phosphate buffered saline (PBS). The fluid should remain in the trachea/lung for three seconds before it is recovery via the connected syringe. The BAL is snap-frozen in liquid nitrogen and stored at -80°C for further analysis. Be aware that the recovered volume could be significantly less than 1 ml.
- Perform blood gas analysis at the end of the experiment. In order to do that, an incision should be made right below the sternum. Hold the sternum with forceps and extent the incision along the rib cage. Next, the diaphragm is incised at the edges and is cut out from the ribs. Now there is an open view into the lower aperture of the thorax. Lift the sternum up with forceps and open the thorax by long cuts at the right and left side (as lateral as possible) so that the complete anterior thorax wall is turned up-wards. This should be done, while the experimental animal is still mechanically ventilated. The left ventricle is punctured using a 27 ½G needle and arterial blood analysis is performed using the i-STAT System (Abbott, USA). If the arterial blood gas analysis should be performed, a BAL cannot be obtained, since this will be a significant confounder to the results.
- Alternatively to method above, arterial blood samples can be collected via the carotid artery catheter. However this should be done before the BAL is obtained.
- Excise the lungs en-bloc by pulling up the heart and cut the trachea. Have a piece of tissue ready to absorb blood, so the surgical site is visible. Pull the heart in the direction of the abdomen and carefully cut along the spine to mobilize all thoracic organs. Cut the aorta, remove the thoracic organs and place them on a clean surgical table.
- Cut away the heart and the major vessel of the tissue sample. Make sure that there is no thymus tissue still attached to the lung. Separate the lungs with a scissor and place in individual tubes and snap-freeze. Store at -80°C for further analysis.
4. Measurement of lung injury
We recommend using the following outcome parameters to assess the extent of lung injury: Perform an albumin ELISA (Bethyl Laboratories, USA) and a myeloperoxidase (MPO) ELISA (Hycult Biotechnology, USA) to assess the extent of barrier dysfunction and the amount of inflammatory cells in the BAL fluid. Perform an MPO ELISA also form the lung tissue. If wet-to-dry ratio is to be measured we do not obtain BAL fluid and the pulmonary circulation is not flushed (see 3.3). Measure the weight of the lungs after excision. Then lungs are lyophilized for 48 h and lung tissue again is measured. Then the wet-to-dry ratio is measured as mg of water per mg of dry tissue (5).
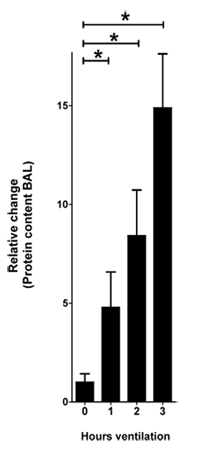
Figure 1. Protein content in the BAL in response to VILI. Mice were anesthetized with pentobarbital, mechanical ventilation
was instituted and mice were ventilated using pressure-controlled settings (inspiratory pressure of 45 mbar, positive end-exspiratory pressure
3 mbar, 100% inspired oxygen concentration). After 0, 1, 2 and 3 hours of ventilation BAL was harvested and the protein content was quantified using a
bicinchoninic acid assay (BCA assay). The relative change of the protein content is shown normalized to 0 hours of ventilation
(n=4 per group, * indicates p < 0.05 compared to control, mean ±SEM)
