This procedure has been approved by the Institutional Ethics Committee and is in line with the Declaration of Helsinki and guidelines for human research.
1. Materials
NOTE: For each tDCS session prepare the following materials (Figure 1).
- Obtain a tDCS device – use only a battery driven tDCS device or a mains-connected optically isolated tDCS device. The device should function as a constant current stimulator with a maximum output limited preferably to a few milliampere range. The device must have regulatory approval for human use.
- Obtain rubber electrodes – use either 5 cm x 5 cm square-shaped or 25 cm2 round-shaped electrodes. These electrodes will have the current densities between 0.06 mA/cm2 and 0.08 mA/cm2 for currents of 1.5 mA-2 mA, respectively.
- Prepare sponge pockets that fit the rubber electrodes. If the sponge pocket is too large it will increase the contact surface to the skin.
- Prepare saline solution (standard 0.9% NaCl).
- Prepare alcohol (70%).
- Obtain an adjustable silicone cap – head straps can be used as well, however EEG silicone caps can be better adjusted to the size and the shape of participants' head and are therefore more comfortable for electrode placement.
- Obtain measuring tape (flexible; plastic or ribbon).
- Obtain a skin marker – skin marker pencils or various makeup products (e.g., eye pencil or eyeshadow crayon), the later can be even more convenient as they are dermatologically tested and easily removable.
- Obtain cotton pads.
- Obtain comb and single-use mini silicon hair bands.
- Obtain a syringe or plastic pipette.
- Prepare a protocol sheet – fill-in form for basic information about the session i.e., participants ID, study ID, date, times, notes, etc (see Appendix for an example).
- Prepare a table with pre-calculated head measures to help with electrodes' placement.
NOTE: To speed-up the process and to reduce the possibility for errors, it is advisable to have this table ready in advance. The measurement is based on 10-20 EEG electrode placement system; the values used for calculations are nasion-inion/left-right-preauricular distances (see below). The table gives 20% values for a range of distance values. We have found it as the most convenient to have the table embedded into the protocol sheet (Appendix). - Prepare questionnaires. For each session, collect data on sensations and side effects before and after tDCS; sensations and the level of (un)pleasantness during tDCS; mood and general subjective state i.e., freshness/tiredness.
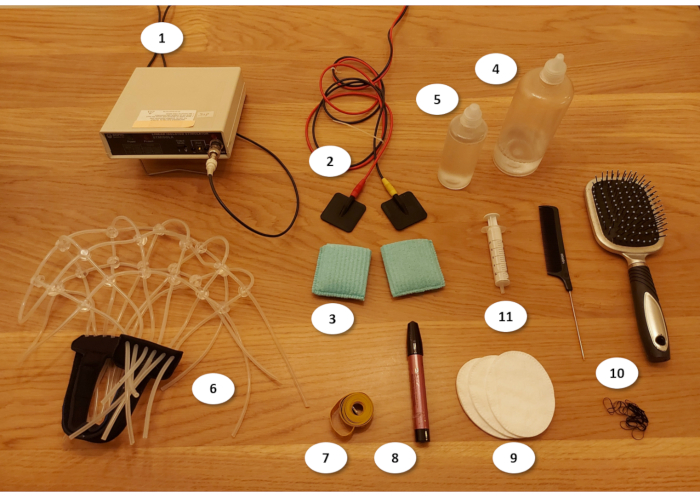
Figure 1: Materials for tDCS experiment (see text for details). 1) tDCS device; 2) electrodes; 3) sponges; 4) saline solution; 5) alcohol; 6) silicone cap; 7) measuring tape; 8) skin pencil; 9) cotton pads; 10) combs and silicon hairbands; 11) syringe Please click here to view a larger version of this figure.
2. Programing stimulation protocols
NOTE: Exact steps in programming tDCS protocol differ across tDCS systems/devices. However, all tDCS devices provide basic features – the ability to produce constant current with desired stimulation intensity, the ability to gradually ramp up and down, and a method to set the duration of stimulation. The more advanced protocols such as theta-oscillatory tDCS require devices/systems that allow for custom-built stimulation protocols.
- Constant anodal tDCS
- Define the standard constant anodal tDCS protocol (Figure 2A) as: (1) fade-in period of 30 seconds, when current intensity is gradually ramped up from 0 mA to the target intensity (we typically use 1.5 mA, but other intensities can be used as well, providing they stay within safety limits); (2) stimulation period during which the constant current of the target intensity (e.g., 1.5 mA) is delivered; and (3) fade-out period of 30 seconds when current intensity is gradually decreased to 0 mA.
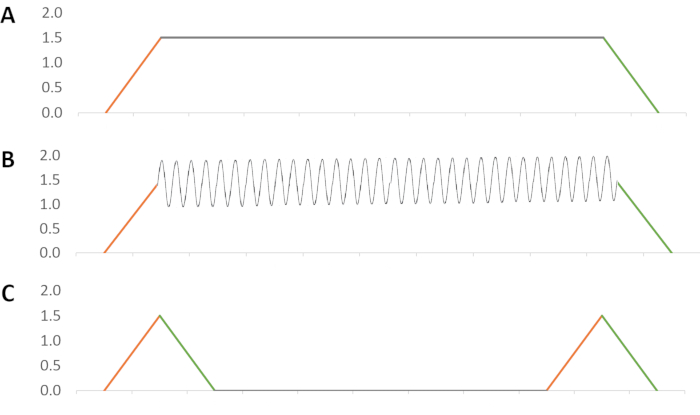
Figure 2: tDCS protocols: (A) Constant anodal tDCS; (B) Theta oscillatory tDCS; (3) Sham tDCS. Fade in period is marked orange; fade out period is marked green. Please click here to view a larger version of this figure.
- Theta oscillatory tDCS
- Theta-oscillatory tDCS delivers current of varying intensity but does not switch polarities (Figure 2B). Therefore, define the waveform in which the current is delivered as following: (1) fade-in period of 30 seconds, when current intensity is gradually ramped up from 0 mA to the target intensity (e.g., 1.5 mA); (2) the stimulation period of 19 minutes in which the current oscillates around the target intensity within a pre-defined amplitude range (we use oscillations of ± 0.5 mA of the target intensity) in a selected frequency (we typically use 5 Hz frequency as representative for theta rhythm); and (3) fade-out period of 30 seconds to bring the current intensity to 0 mA.
NOTE: This protocol can be generated by any experimental control software (e.g., CED Signal) and delivered through an intelligent interface (e.g., CED 1401 range of devices) that is compatible with tDCS device which is to be used. Some more advanced dedicated transcranial electric stimulation (tES) systems besides tDCS can deliver alternating current (tACS) and random noise stimulation (tRNS) too. They can also be used to generate the oscillatory tDCS protocol. For example, in StarStim the theta-oscillatory tDCS protocol are defined as a linear combination of tDCS (1.5 mA) and tACS (±0.5 mA, 5 Hz). This type of protocol can be personalized in a sense that not all participants receive oscillatory stimulation in the same frequency (i.e., 5 Hz), but that the frequency is adjusted to the dominant frequency within theta band for each person (e.g., Person 1: 5 Hz, Person 2: 6 Hz, Person 3: 4.5 Hz, etc.).
- Theta-oscillatory tDCS delivers current of varying intensity but does not switch polarities (Figure 2B). Therefore, define the waveform in which the current is delivered as following: (1) fade-in period of 30 seconds, when current intensity is gradually ramped up from 0 mA to the target intensity (e.g., 1.5 mA); (2) the stimulation period of 19 minutes in which the current oscillates around the target intensity within a pre-defined amplitude range (we use oscillations of ± 0.5 mA of the target intensity) in a selected frequency (we typically use 5 Hz frequency as representative for theta rhythm); and (3) fade-out period of 30 seconds to bring the current intensity to 0 mA.
- Sham tDCS
- Use a sham protocol with the same duration as constant/oscillatory tDCS (Figure 2C). Namely, define it as: (1) first fade in/out period in which the current is gradually ramped up to target intensity (e.g., 1.5 mA) and gradually ramped down to 0 mA during the first 60 seconds (2) 18 minutes of 0 mA, and (3) the second fade in/out period which again lasts 60 seconds.
NOTE: An alternative approach would be to use very low current intensity over the entire stimulation period (20 min). This type of sham protocol is programmed the same as the anodal stimulation (only the current intensity is set to (0.1 mA) and is designed to produce cutaneous sensations but the intensity is too week to produce any physiological effects33.
- Use a sham protocol with the same duration as constant/oscillatory tDCS (Figure 2C). Namely, define it as: (1) first fade in/out period in which the current is gradually ramped up to target intensity (e.g., 1.5 mA) and gradually ramped down to 0 mA during the first 60 seconds (2) 18 minutes of 0 mA, and (3) the second fade in/out period which again lasts 60 seconds.
3. Electrode placement (Figure 3)
- DLPFC electrode montage: For stimulation of the DLPFC, place the target (anodal) electrode on either F3 (left) or F4 (right) of the international 10-20 EEG system. Place the return electrode (cathodal) on the contralateral cheek – i.e., right cheek for F3 anode and left cheek for F4 anode.
- PPC electrode montage: For stimulation over PPC, place the target (anodal) electrode on either P3 (left) or P4 (right) of the international 10-20 EEG system. Place the return electrode (cathodal) on the contralateral cheek same as in DLPFC montage.
- The target electrode placement
- To locate F3 on participants' head
- Use the measuring tape to measure the distance between nasion (the deepest point of the nasal bridge) and inion (the most pronounced point of the external occipital protuberance) going over the top of the head. Mark the halfway distance with the skin marker with a thin line.
- Measure the distance between the ears (use preauricular points as references) going over the top of the head and mark the halfway distance with a thin line.
- Find the vertex or midline central position, referred as Cz, at the intersections of the two midlines. Mark it clearly with the skin marker.
- Measure again the nasion-inion distance, but this time going over Cz, and note the distance as measure A. Measure again the distance between the ears, this time going over Cz, and note the distance as measure B.
- Calculate 20% of distance A, and 20% of distance B (or see Protocol sheet for pre-calculated values).
- Move 20% of distance A forward from Cz along the nasion-inion line to reach Fz (midline frontal) and mark the spot.
- Move 20% of distance B leftward from Cz along the inter-auricular line to reach C3 (left central) and mark the spot.
- Move 20% forward form C3 (in parallel with the nasion-inion line), and 20% leftward form Fz (in parallel with the inter-auricular line), to reach F3 at the intersection. Mark F3 with the skin-marker and place the center of the electrode at the spot.
- To locate F4, follow the same procedure only on the right side of the head.
- To locate P3 on participants' head
- Follow the steps 3.3.1.1-3.3.1.5 as outlined above (find Cz, note distance A and B, calculate 20%).
- Move 20% of distance A backward from Cz along the nasion-inion to reach Pz (midline parietal) and mark the spot.
- Move 20% of distance B leftward from Cz along the inter-auricular line to reach C3 and mark the spot.
- Move 20% backward from C3 (in parallel with the nasion-inion line), and 20% leftward from Pz (in parallel with the inter-auricular line), to reach P3 at their intersection. Mark P3 with the skin-marker and place the center of the electrode at the spot.
- To locate P4, follow the same procedure only on the right side of the head.
- To locate F3 on participants' head
- Return electrode placement
- After securing the target electrode with the adjustable silicon cap (see step-by step procedure), insert the return electrode below the chin band to secure the contact of the electrode with the contralateral cheek.
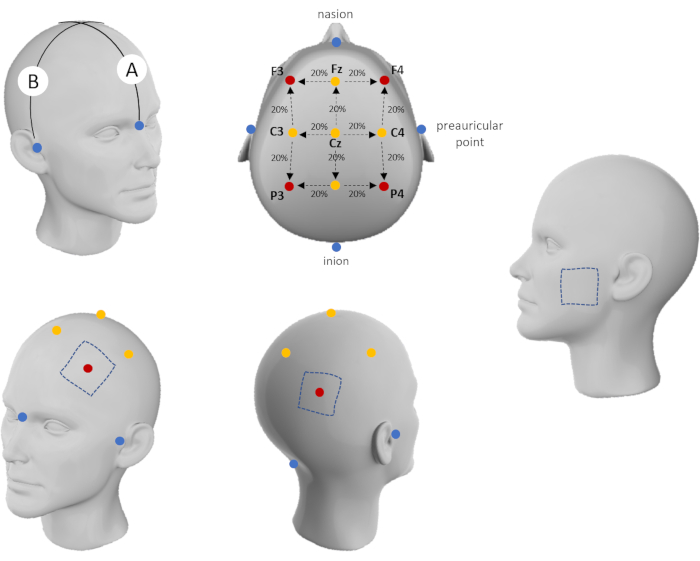
Figure 3: Electrode placement scheme. Please click here to view a larger version of this figure.
4. Step-by-step procedure
- Before the tDCS session
- Check if each participant satisfies the inclusion criteria as defined in ethical approval for the study (see Appendix for the most common inclusion/exclusion criteria).
- Ask the participant to fill in the Participant information sheet (including all the relevant information such as age, gender, nicotine/alcohol consumption, etc.34).
- Follow the institutional review board ethical guidelines, and ask participant to sign informed consent. Use this opportunity to explain the basic aspects of the procedure they will undergo and answer any questions the participants may have.
- Depending on the study design, perform baseline cognitive assessment (memory and/or other cognitive functions).
- tDCS set-up and stimulation
- Seat the participant comfortably in a chair.
- Ask participant to fill out pre-tDCS sensations checklist and to report on overall state (i.e., current mood; freshness/tiredness – these can be assessed either as a single Likert-type item or using standardized questionnaires such as Brief Mood Introspection Scale35).
- Take head measures using a measuring tape.
- For locating the DLPFC or PPC follow the procedure described above (electrode placement). Write down the measures in the Protocol sheet for each participant. These can be used to check against when taking measurements in subsequent sessions.
- To increase conductance, move away participant's hair from stimulation site (use comb and hair bands for participants with long hair).
- Inspect for any signs of skin damage at the place of stimulation. Avoid positioning electrodes over damaged skin.
- Clean the surface of the skin where electrodes will be placed using alcohol-soaked cotton pads to remove grease, dirt, etc. and let it dry (use a makeup removal product if the participant has heavy makeup on the cheek).
- Put the silicon cap on the participant's head and secure it with the chinstrap. Do not make the cap tight (this will be done later).
- Soak the sponge pockets with saline solution and put the electrodes inside them. The sponges should be moist but not dripping; usually 10-15 mL of saline solution per sponge is enough. If the sponges are too dry this will cause high resistance and result in poor conductivity, even losing the circuit connection.
NOTE: Most of the tDCS devices have the resistance indicators; however, the sponges should be occasionally inspected for moisture. On the other hand, if the sponges are excessively wet it can cause the current to shift across the head during stimulation. It is recommend having sponges medium wet and use a syringe to add more saline solution during the experiment if the sponges become too dry. - Put the sponge electrode under the silicon straps and position the center of the target electrode on the marked head-location. Set the return electrode on the contralateral cheek. Use the silicon straps to adjust the cap to the participant's head-size and shape. The cap should be tight so the electrodes cannot move, but still comfortable for the participant.
- Turn on the stimulator, select and run predefined tDCS protocol (active anodal stimulation or sham).
- Ask the participant to relax and let them report how they feel during the first few minutes of stimulation (1-3 minutes). Explain that the sensations will slowly fade away as they get used to it or when they start focusing their attention on some other activity.
- To avoid unstructured activities that can interfere with the stimulation effects, use light cognitive engagement during tDCS. For example, participants can perform practice trials of cognitive tasks or engage in easy memory games during stimulation (starting after 3-5 minutes of stimulation). This type of cognitive engagement during stimulation has the potential to promote tDCS effects and will help participants to keep the mind off the tDCS-induced skin sensations.
- Ask the participant to report how they feel multiple times during stimulation (e.g., to report the level of unpleasantness on a 10-point scale every 5 minutes of stimulation, 1 – completely absent, 10 – very intensive). Higher levels of unpleasantness (>6) could be expected during fade-in fade-out periods in some participants. If the level of unpleasantness remains high after 5 minutes abort the stimulation.
- After the pre-defined protocol run has elapsed, turn off the stimulator.
- Remove the sponge electrodes first, and then remove the silicon cap.
- Ask the participant to fill out post-tDCS sensations checklist and to report for any side effects not already listed.
- Clean the skin on the places where it was marked and inspect the skin for any changes. If there is a skin reaction (e.g., local vasodilation i.e., skin redness on the cheek), monitor as it fades away as it is usually a transient reaction in participants with sensitive skin, and should disappear within 10-15 minutes.
- Memory assessment
- To standardize the assessment across participants, use computerized assessment tools i.e., memory tasks with automatic scoring. Several WM tasks (e.g., verbal and spatial 3-back task) and AM tasks (verbal paired learning; face-word cued recall, object location, etc.) can be found here: https://osf.io/f28ak/?view_only=f8d5e8dd71d24127b3668ac3d8769408
- To evaluate the specificity of tDCS effects on memory it is advisable to include control task(s) i.e., tasks tapping other cognitive or motor function.
- Ending the experimental session/study
- After the (last) experimental session in the study ask participant to try to guess the sessions in which they have received real and sham stimulation. Note all responses and see whether obtained proportions are higher than chance probability. If not, the blinding was successful. If participants were able to differentiate real from sham stimulation analyze the data for those that guessed correctly and those that did not to check if the unsuccessful blinding affected the tDCS effects.
- In line with ethical guidelines, debrief the participants in detail after their involvement is completed.
- After the experimental session
- Wash the sponges with running water and soap so that the saline solution is fully washed away. Let the sponges to dry completely before putting them away.
- Use warm water and alcohol to clean all reusable materials including comb, silicone cap and measuring tape.
- Make notes on all unusual, unexpected, or unplanned events that might have happened during the session – including any equipment malfunctions, relevant comments made by the participant, interruptions, etc.
The described protocol has been successfully used to enhance memory performance in several studies in our laboratory. However, similar protocols have been used in other research laboratories as well (e.g., see36,37).
When it comes to working memory, our results have shown that 20-minutes of right frontal tDCS (F4 location; constant current of 1.8 mA) enhanced verbal WM, while the same stimulation protocol applied over left parietal cortex (P3 location) resulted in better spatial WM performance. In contrast, no significant effects were found when the same stimulation protocol was applied over the left frontal (F3) and right parietal (P4) cortices. Figure 4 shows the representative results of modeling of the electric field generated by tDCS as well as the performance measures following active and sham tDCS based on the data reported in Živanović et al., 202138.
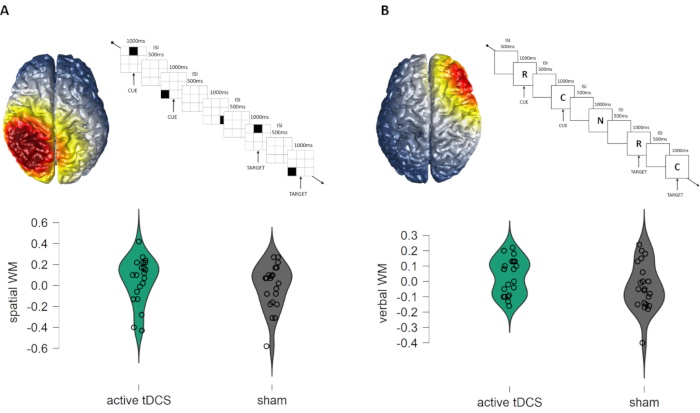
Figure 4: (A) Effects of constant anodal tDCS of left PPC (P3-contralateral cheek montage) on spatial working memory performance (spatial 3-back task); (B) Effects of constant anodal tDCS of right DLPFC (F4-contralateral cheek montage) on verbal WM performance (verbal 3-back task). The figure shows simulation of electric fields induced by tDCS, outline of the task trials, and the within-subjects performance across active and sham condition (the values are centered to the order of the session to account for counterbalancing i.e., positive values indicate above-average performance, while negative values indicate below average performance at session). The simulation of local electric fields generated by the electrode set up is performed using COMETS2 MATLAB toolbox 41. Please click here to view a larger version of this figure.
The effects of parietal tDCS on associative memory have been consistent and robust. That is, in the series of within-subject experiments we have shown that 20 minutes of tDCS over left PPC (P3 location; constant current of 1.5 mA) improves memory for face-word associations27,39,40. Figure 5 shows representative task and results. In addition, comparable effects were observed on AM task assessing the object-location associations when right PPC (P4 location) is stimulated using the same constant tDCS protocol40.
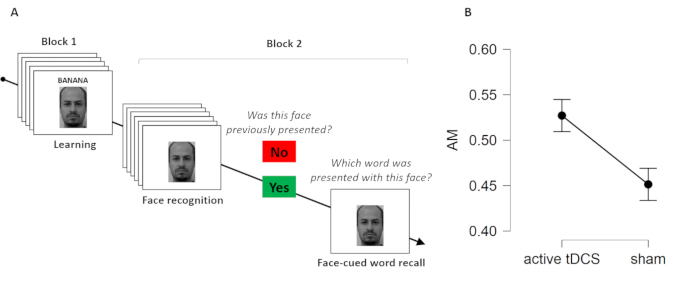
Figure 5: Effects of constant anodal tDCS of left PPC (P3-contralateral cheek montage) on associative memory performance (A) Face-word pairs task; (B) Effects of constant anodal tDCS of left PPC (P3-contralateral cheek montage) on associative memory performance (proportion of correctly recalled words on cue). Please click here to view a larger version of this figure.
The more advanced protocols such as theta-oscillatory tDCS have been less extensively studied, however the study by Lang and colleagues26 as well as recent study conducted in our laboratory27 showed improvement in face-word AM following theta-oscillatory tDCS protocol in comparison to sham. The animated figure shows simulation of the electric field induced by theta oscillatory tDCS over left PPC.
