Respiratory system mechanics measurements. Table 4 shows typical results from naïve A/J mice obtained at baseline and following methacholine-induced bronchoconstriction (12.5 mg/ml) using either of the two flexiVent generations supported by flexiWare 7 software. Mechanics of the respiratory system, i.e. under closed chest conditions, were assessed by alternating perturbations of the single and broadband frequency forced oscillation families in a closely spaced manner (SnapShot-150, Quick Prime-3, respectively). Since ventilation is paused during measurements, the Quick Prime-3, which covers a similar frequency range as the Prime-8 but has a shorter duration (3 vs 8 sec), was selected in order to shorten the apneic period, minimize the effect of the perturbation on blood gases and provide a better resolution of the response. Parameters associated with each perturbation were calculated automatically by the operating software. Results illustrate that the two generations of the flexiVent system produced equivalent measurements of respiratory mechanics.
Site of lung response. Distinguishing the site of lung response allows the investigator to further pinpoint affected regions as well as to identify potential points of pharmacological intervention6. For example, naïve A/J mice show an increase of baseline resistance when the end expiratory pressure against which measurements are made is increased from 3 to 9 cmH2O (Figure 6A, SnapShot-150). In the present example, the use of broadband FOT measurements (Quick Prime-3) provided details to clarify the basis for the change in resistance: The change in end expiratory pressure resulted in a decrease in the airway resistance (RN) consistent with the bronchodilating effects of a higher lung volume and the larger inflation pressure (Figure 6D) and an increase in tissue damping (G; Figure 6E), a parameter closely related to tissue resistance that reflects tissue viscoelasticity and possibly the resistance of the small airways7. The latter is known to increase with increasing lung volume.
Airway hyperresponsiveness. Following chlorine gas exposure, airway responsiveness to inhaled methacholine increases compared to air exposure in Balb/c mice as a result of airway damage4 (Figure 2). Chlorine is known to induce oxidative stress, leading to destruction of structural cells in the airways, in particular epithelial cells, and inducing recruitment of inflammatory cells. As represented in Figure 5, changes in all parameters describing respiratory system mechanics can be seen in response to increasing methacholine challenges. In comparison to air-exposed mice, mice exposed to chlorine gas displayed greater maximal responses at all FOT parameters (Figure 5A, 5B, 5D-5F) as well as a statistically significant leftward shift of the concentration-response curve exemplified by a reduction of the concentration of methacholine required to cause a doubling in resistance and elastance (PC200; Figure 5C). Those results illustrate, respectively, airway hyperresponsiveness and hypersensitivity to inhaled methacholine following exposure to chlorine gas.
Other measurements. In addition to FOT, the flexiVent system can also be used to collect other types of lung function8-10 or cardiovascular11 measurements. Figure 7 displays a representative stepwise, pressure-driven pressure-volume curve in naïve A/J mice under baseline conditions. The upper portion of the deflation limb of the curve is fit to the Salazar-Knowles equation12 and parameters are automatically calculated by the software.
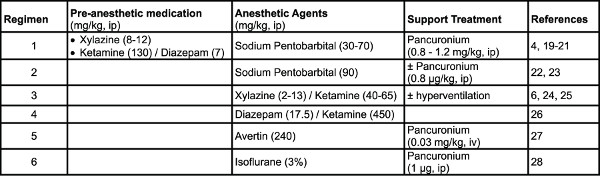
Table 1. Examples of anesthetic regimens used in mice. Click here to view larger table.
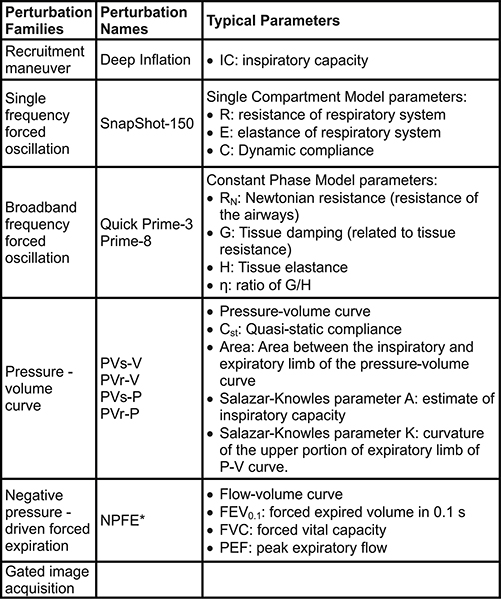
Table 2. Perturbations used for lung function measurements in mice. *Extension required to the system. The subject also needs to be in a closed plethysmograph chamber during measurements. Click here to view larger table.
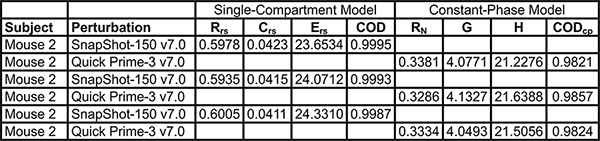
Table 3. Example of exported parameters from the single and broadband frequency forced oscillation perturbation families. Click here to view larger table.
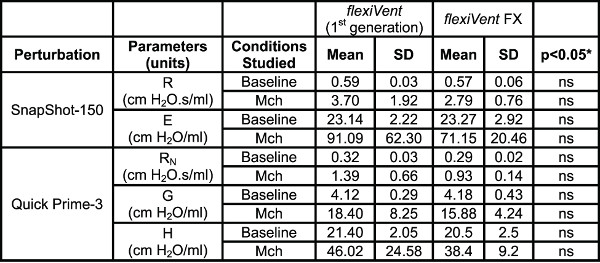
Table 4. System Comparison. Comparison of lung mechanics parameters collected using the two generations of the flexiVent system operated by flexiWare 7 software. Results were generated in naïve A/J mice (n=5/group) at baseline and following methacholine-induced bronchoconstriction (Mch 12.5 mg/ml). *Groups were compared using a two-way ANOVA for repeated measurements and the log10 of individual responses for homogeneity of variances (GraphPad Prism, version 5.03; GraphPad Software, San Diego, USA).
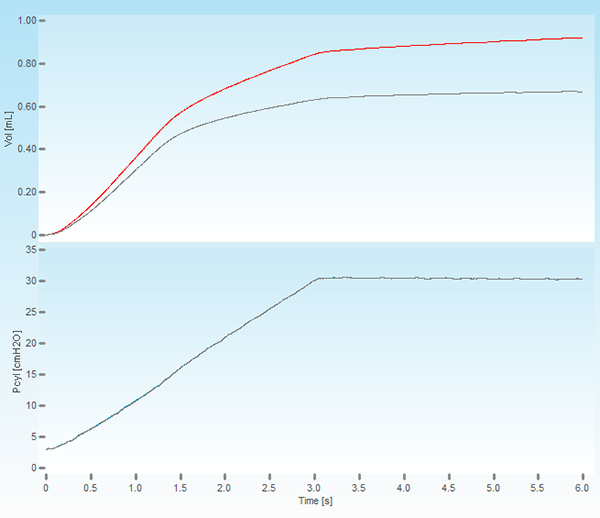
Figure 1. Screenshot of a deep lung inflation. The upper panel shows the volume displaced by the piston of the ventilator (red trace) and the volume delivered to the subject (grey trace). The lower panel displays the cylinder pressure increasing to a set pressure of 30 cmH2O over a period of 3 seconds and held constant for the same time period.
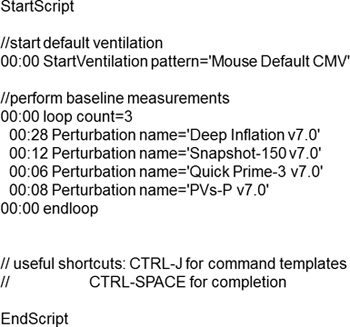
Figure 2. Example of a typical script used to assess respiratory system mechanics at baseline.
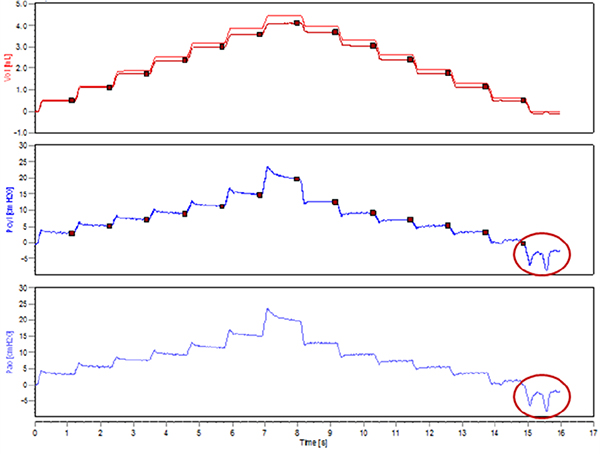
Figure 3. Spontaneous inspiratory efforts during the execution of a stepwise pressure-volume curve.
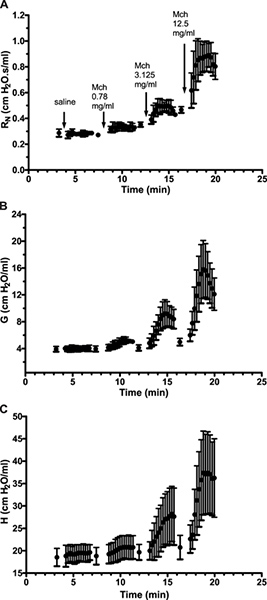
Figure 4. Time-course response following increasing inhaled methacholine challenges. Results are expressed as the mean (± standard deviation) of a group of 5 naïve spontaneously hyperresponsive A/J mice. Click here to view larger figure.
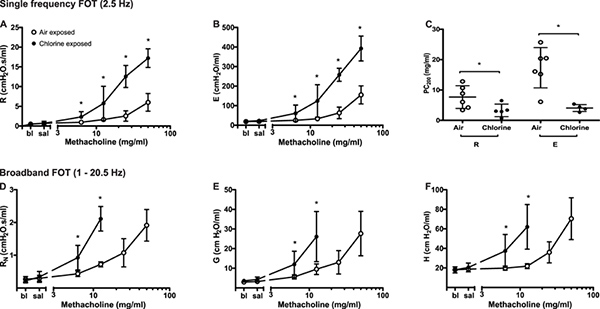
Figure 5. Changes in respiratory system mechanics following increasing methacholine challenges in chlorine- and air-exposed Balb/c mice. Peak value was identified for each parameter in every subject and experimental condition. Group averages were then calculated (mean ± standard deviation; n=4-6). Differences between groups were assessed by analysis of variance using the log10 of individual responses for homogeneity of variances. The concentration of methacholine producing a doubling of baseline (PC200) was obtained by fitting a second order polynomial to individual dose-response curves and interpolation of the fitted curve. Data points are missing in D, E and F in the chlorine-exposed mice at the two highest methacholine concentrations due to insufficiently high coefficients of determination reflecting a poor fit of the mathematical model to the data. Click here to view larger figure.
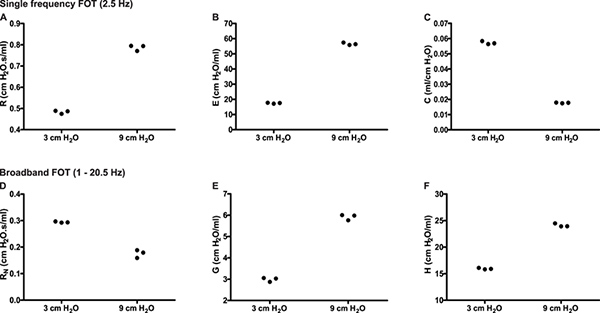
Figure 6. Partitioning of the respiratory response into airway and lung tissue mechanics. Experimental trace from a naïve A/J mice illustrating single (2.5 Hz) and broadband (1-20.5Hz) frequency forced oscillation measurements of respiratory mechanics in triplicate at two different end expiratory pressures (3 & 9 cmH2O). Click here to view larger figure.
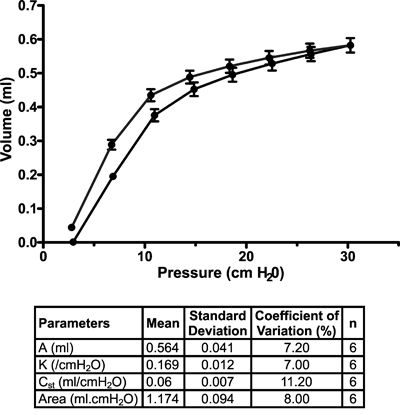
Figure 7. Pressure-volume curve in naïve A/J mice under baseline conditions. Pressure-volume curves were generated using a stepwise pressure-driven perturbation (PVs-P) to ensure that each mouse lungs were inflated to the same pressure, independently of their condition. Salazar-Knowles equation parameters extracted from individual pressure-volume curves were also averaged and reported in a table format. Results are expressed as the mean ± standard deviation (n=6).
