1. Instrumentation
Vector TDI is based on estimating the resultant velocity vector from Doppler velocity measurements taken from two or more independent directions. An ultrasound system with a research interface was used for developing vTDI. The research interface allowed low level beamforming and pulse sequence control using a software development kit (SDK). A 5-14 MHz linear array transducer, consisting of 128 transducer elements and with a 38 mm field of view was used. The research interface was employed to split the array transducer into two transmit and receive apertures and steer the receive beams by 15° with respect to the normal. The transmit beam was focused in the region of interest (e.g. muscle belly). Transmit and receive apertures were set to 32 elements.
Eight subjects, 4 men and 4 women (29.7±6.5 years) were recruited in this study. Kinematic measures from the subjects of the right lower extremities were captured using an eight-camera motion capture system with high speed capability and a sampling rate of 200 Hz. Ground reaction force data during the experiment were obtained through two force plates sampling at 2,000 Hz.
A high-speed camera mounted on a tripod and placed at 2 m from the subject, was used to capture the drop landing at 500 frames/sec.
2. Subject Preparation
- Ask the subjects to wear a pair of shorts, sports bra or a short t-shirt and running shoes.
- Instruct the subjects to perform a 10 min self-directed warm-up and stretching prior to the data collection. This is to avoid any abnormal muscular contractions and reduce the scope of any muscle cramps.
- After the warm-up session, place reflective markers on specific landmarks on the body. Specifically, place calibration markers on the greater trochanters, bilateral medial and lateral knee and medial and lateral malleoli. Place tracking markers on the posterior and anterior superior iliac crests, and place clusters on the thighs and shanks, and five markers on each foot 19-20.
- Direct the subjects to the stand in the center of the focus area of the 3D cameras to obtain a static trial. The participants must stand on the force plates with their arms across their shoulders, to obtain static 3D motion capture data.
- Then, place the ultrasound transducer in a transducer holder and ensure good contraption, to avoid dislodging of the ultrasound transducer from the transducer holder. The transducer holder was made using Lexen polycarbonate and moldable plastic.
- To ensure good contact with the skin and ultrasound transducer, apply generous amount of ultrasound transmission gel on the transducer.
- Place the ultrasound transducer along with the transducer holder on the thigh of the subject to image the rectus femoris muscle in the longitudinal axis. The transducer must be placed halfway between the anterior iliac spine and the lateral epicondoyle to image the belly of the rectus femoris muscle. Before securing the ultrasound transducer and the transducer holder to the leg, obtain an axial slice of the quadriceps muscle group. Using this as a guidance, make sure the ultrasound transducer is now imaging the rectus femoris and does not move more lateral or medial, to avoid imaging the vastii muscle group.
- Now, use a cohesive self-adhesive bandage to secure the transducer holder onto the subject’s thigh. Make this procedural step does not block or cover the reflective markers. The self-adhesive bandage must not be lax or excessively tight. Lax bandaging will risk the ultrasound transducer to fall during the drop-landing task and an excessively tight bandaging will cause discomfort, disrupt superficial blood flow and possibly alter drop landing dynamics.
- Place the high speed camera at least 2 m away from the subject in the sagittal plane to collect videos at a 500 frames/sec. Focus the camera lens to ensure that the entire drop landing sequence of the subject can been captured.
3. Experiment Protocol
- Once all the markers and the ultrasound transducer are secure, ask the subjects to stand on a platform of height 30 cm place at 50 cm from the force plates. Ensure that the area around the platform (about 2.5 m) is clear of any objects that could hinder the drop landing task or injure the subject. This includes the ultrasound transducer cord.
- Instruct the subjects to place their hands on their hips prior starting the drop landing task and during the entire drop landing sequence.
- Start the data collection for ultrasound, 3D motion capture, force plates and the high speed camera prior to start of the drop landing task. Synchronization between the different instruments can be achieved by using a single key press to start all the data acquisition. A pressure sensor attached to the keyboard can be used to generate a synchronizing trigger signal when a specific key is pressed.
- Direct the subject to perform the drop-landing task from the platform and land with both legs, simultaneously. Ensure that the subjects drop from box instead of jumping from it. No specific instructions are provided regarding landing technique.
- Stop the data collection once the subject has fully stabilized and completed the drop landing sequence.
- Repeat this protocol five times per subject.
4. Ultrasound Data Analysis
- Export and store the raw data from the ultrasound system to a computer.
- The raw radiofrequency (rf) ultrasound data from each receive beam is digitized at 40 MHz. Process the data using MATLAB.
- Perform quadrature demodulation on the RF data to remove the carrier frequency. Remove stationary and low-frequency clutter by filtering the quadrature data from each the receive beams and for each depth using a 20 Hz high pass filter.
- Estimate the velocities along both receive beams using the conventional autocorrelation velocity estimator 21.
- Combine the individual velocity waveforms to obtain lateral (along the transducer) and axial (perpendicular to the transducer) velocity waveforms throughout the drop landing sequence, as seen in Figure 1.
- Obtain the magnitude of the resultant velocity vector from the individual velocity components using equation 1 as described previously 22:
where β is the beam steering angle, f1 and f2 are the two received frequency components and ft is the transmit frequency. - Calculate the lateral and axial strain rate de/dt using the spatial gradients in the lateral and axial velocities.
where V2 and V1 are instantaneous velocities estimated at two spatial locations separated by a distance L. - Calculate the axial and lateral strain, e, by integrating the axial and lateral strain rate respectively.
5. 3D Motion Capture Data Analysis
- Export the 3D motion capture data to a computer for further analysis.
- Using the static standing trial, create a kinematic model (pelvis, thigh, shank, and foot) using 3D motion capture software with a least-squares optimization 23.
- Use this kinematic model to quantify the motion at the hip, knee, and ankle joints.
- Filter the reflective marker trajectories and ground reaction forces using a 4th order low-pass Butterworth filter with a cutoff frequency of 7 Hz and 25 Hz, respectively using 3D motion capture software.
- Calculate 3-D joint forces and moments from the kinematic and ground force data using a standard inverse dynamics analysis, using segment inertial characteristics estimated for each participant as per the methods of Dempster. Inter-segmental joint moments are defined as internal moments (e.g. a knee internal extension moment will resist a flexion load applied to the knee).
6. High Speed Camera Data Analysis
- Export the videos from the high speed camera data to a computer for analysis and comparison with ultrasound and 3D motion capture kinematic data.
- Play the movie at 15 frames/sec and observe the drop landing dynamics.
- Then, quantify the movement of the transducer holder and the displacement of the ultrasound transducer during the entire drop landing trial by tracking the visible markers on the anatomical landmarks using the high speed video data. Assessing the drop landing dynamics can also be done simultaneously to better understand the different launch and landing styles.
Representative results from our previous work demonstrating the methods are presented below. While the methods utilized in our current research integrate imaging and motion capture, the representative results presented below are from studies where these measurements were performed separately.
I. Ultrasound (vTDI)
Using the data from the 3D motion capture and the high speed camera, the pattern of subject’s jump, landing and stabilization phases were studied for each trial. The axial and lateral rectus femoris muscle velocities from vTDI were compared to data collected from 3D motion capture and high speed camera. Using this data, the temporal characteristics of the axial and lateral rectus femoris muscle velocities throughout the drop landing sequence were studied. Positive lateral velocities correspond to eccentric contraction of the rectus femoris muscle during knee flexion, while negative lateral velocities correspond to concentric contraction of the muscle during knee extension. This is illustrated in Figure 2. The entire drop-landing sequence for all subjects lasted approximately 1.45±0.27 seconds.
For each subject, the axial and lateral muscle velocities showed a strong repeatability between trials with a slope of 0.99 and R2 = 0.75 (Figure 3). Velocity values for six out of eight subjects were in a similar range of 48-62 cm/sec, while two subjects (both men) had higher velocities. Males (72.96 cm/sec) presented significantly higher muscle velocity than females (48.71 cm/sec), p=0.029, when adjusting for each subject’s individual weight and muscle thickness.
The position of the ultrasound transducer was tracked thought the drop-landing sequence using the high-speed camera. The angle between the line segment made between the trochanter and the cuff (green dashed line segment) and the line segment between the mid-thigh and the cuff (purple dashed line segment) was calculated. A total of 16 trials, with 2 trials per subject (trial 1 & 2 relate to subject 1 and so on) are observed in Figure 4. Minimal angular variation (0.91°±0.54 degrees) of the transducer holder relative to the anatomical markers during landing was observed over all 16 trials. The ultrasound transducer angular variation presented a high repeatability as well (ICC2,1 = 0.90, p<0.05).This shows that the transducer movement during the landing trial was minimal and the velocity measurements were not affected due to any transducer movement.
II. 3D Motion Camera & Force Plates
We primarily focused on knee and hip flexion angles, knee valgus angle, and knee valgus moment. We found that during the initial contact with the ground, subjects had the following kinematic patterns: hip flexion 41°±13 degrees, knee flexion 23°±9 degrees, and knee valgus 0.03°±6 degrees. As they progress during the landing phase, the maximum angles attained were: hip flexion 58°±19 degrees, knee flexion 54°±24 degrees, and knee valgus -4°±8 degrees (Figure 5). Knee valgus moment presented a decrease from 0.03±0.03 to 0.1±0.1 Nm/km from initial ground contact to its maximum during the landing phase (Figure 6).
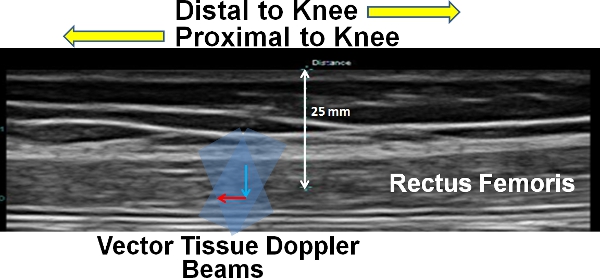
Figure 1. Representation of the vTDI velocity measurement of the rectus femoris muscle. The grey beam represent the two individual transmit and receive beams and the red line represents the lateral velocity component (along proximal-distal direction of the knee) and the blue line represents the axial velocity component (along the thickness of the muscle).
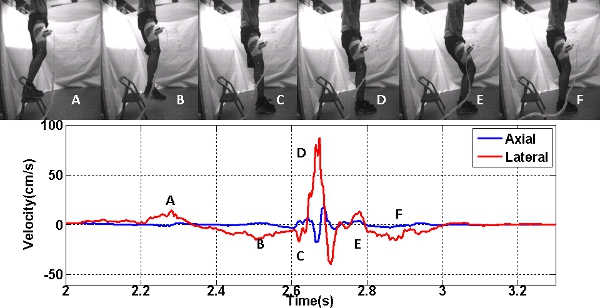
Figure 2. Axial and Lateral velocities during drop landing are compared to the sequence of video frames (upper panel). The lower panel is the axial and lateral velocities, where A corresponds to the initial knee flexion, B corresponds to the knee extension, C corresponds to the toe striking the ground, D corresponds to the heel striking the ground, E corresponds to knee flexion post landing and F corresponds to the knee extension and stabilization.
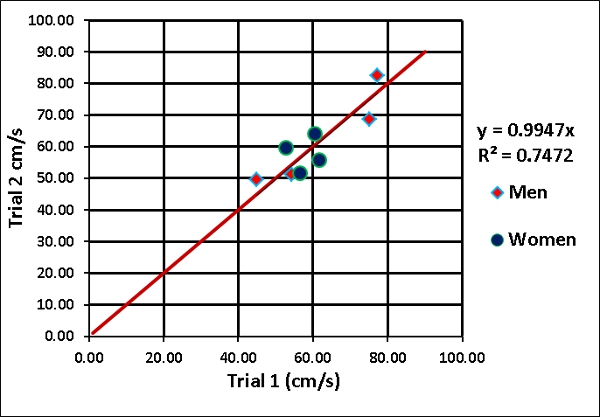
Figure 3. Repeatability of the magnitude of the resultant velocity vector for all 8 subjects (2 trials per subject). Men are denoted in red diamonds and women in blue circles.
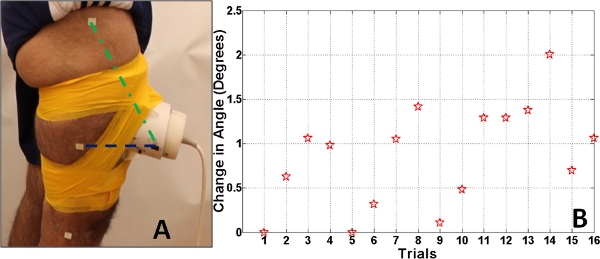
Figure 4. Panel A. The error in the angle between the line segment made by ultrasound transducer holder and the marker on the mid-thigh (purple dashed line segment) and the line segment made by the ultrasound transducer and the marker on the trochanter (green dashed line segment). Panel B. The absolute error in the angle between the line segment made by ultrasound transducer holder and the marker on the mid-thigh and the line segment made by the ultrasound transducer and the marker on the trochanter.
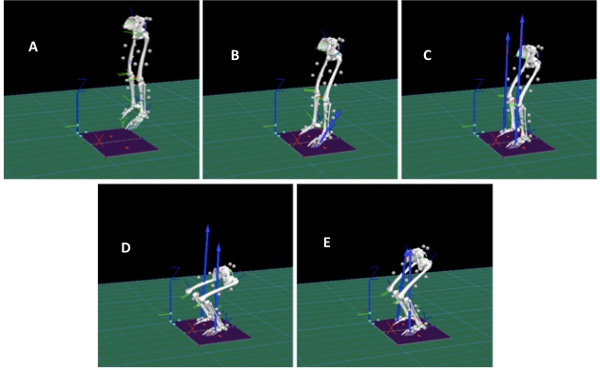
Figure 5. Figure shows the 3D motion capture during the drop landing task. A corresponds to the initial knee flexion for launch from platform, B corresponds to the toe striking the ground, C corresponds to the heel striking the ground, D corresponds to knee flexion post landing and E corresponds to the knee extension and stabilization. Click here to view larger figure.
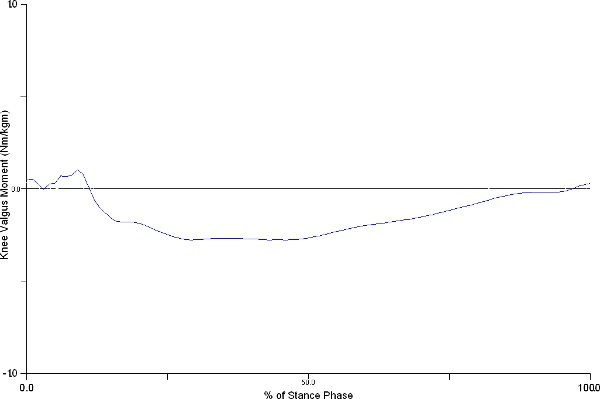
Figure 6. Figure shows representative knee valgus moment changes during the stance phase of drop-jump. Knee valgus moment presented an increase from 0.03±0.03 to 0.1±0.1 Nm/km from initial ground contact to its maximum during the landing phase. Click here to view larger figure.
