1. Participants
- Provide approval for the protocol and informed consent procedures from the University Institutional Review Board.
- Recruit adolescent and young adult UHR participants by using Craigslist (i.e. local classified advertisements on the internet), email postings, newspaper ads, and community professional referrals.
- Recruit healthy control participants by craigslist, flyers and newspaper announcements.
- Advertise that the study looks at healthy development for volunteers with no family history of psychosis and no psychiatric symptoms.
- Exclude healthy controls based on the presence of any category of Axis I disorder or a psychotic disorder in a 1st degree relative.
Note: A psychotic disorder in a first degree relative is intended as exclusion criteria for healthy controls because of the familial or genetic risk of psychosis1.
- Exclude all participants based on criteria consisting of a history of head injury, the presence of a neurological disorder, substance dependence, or a history of taking neuroleptic medication.
- Exclude UHR participants based on the presence of an Axis I psychotic disorder (e.g. schizophrenia, schizoaffective disorder, schizophreniform).
2. Clinical Interviews
- Train interviewers to administer the Structured Interview for Prodromal Syndromes (SIPS) to diagnose a prodromal syndrome and the Structured Clinical Interview for Axis-I DSM IV Disorders (SCID) over a 2 month period.
- Establish inter-rater reliabilities on clinical interviews to exceed the minimum study criterion of Kappa ≥80.
- Define criteria for a prodromal or high-risk syndrome by moderate levels of positive symptoms and/or a decline in global functioning accompanying the presence of schizotypal personality disorder and/or a family history of schizophrenia.
- Compute a total sum score for each category as an indicator of the respective dimensions of symptomatology.
Note: The SIPS gauges several distinct categories of prodromal symptom domains including positive, negative, and disorganized dimensions. - Administer the Structured Clinical Interview for Axis-I DSM-IV Disorders (SCID) to rule out a psychotic disorder diagnosis.
Note: This measure has been demonstrated to have excellent inter-rater reliability in adolescent populations and has been used in several previous studies focusing on adolescent populations with schizophrenia spectrum disorders. - Assess the participant's nicotine usage during the past month. Rate tobacco usage on a 0-5 scale with 0 = abstinent and 5 = 20+ cigarettes per day.
3. Handwriting Task
- Run Neuroscript MovAlyzeR software with a tablet computer and a noninking pen.
- Create an example of LLeeLLee on a notecard (see Figure 1).
Note: The software and stimulus are described previously and have been shown to be valid tools for detecting movement abnormalities in schizophrenia patients and Parkinson's patients15-17.
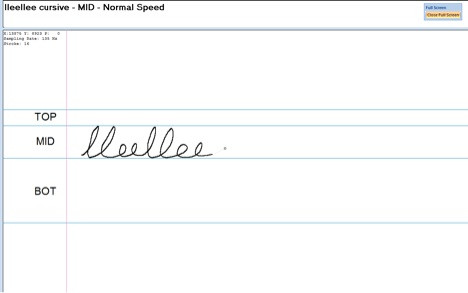
Figure 1. Example of the test condition. Participants are instructed to write the word LLeeLLee in cursive in the MID section. It is helpful to have an example such as this to show the participant so that they understand the instructions.
- Leave the example notecard visible to the participant throughout the experiment. Note: The notecard will help the participant understand the experiment.
- Orient tablet into landscape mode to provide a writing space of 18 cm x 28 cm with a resolution of 1,280 x 800 pixels.
- Allow participants to position computer screen into a comfortable writing position.
- Set the sampling rate in the software to the measured sampling rate (e.g. 100-200 Hz).
- Instruct participant to write the word LLeeLLee in cursive in the 2 cm guidelines with the dominant hand.
Note: The condition is programmed to divide the writing surface into 4 regions. There are horizontal lines measuring 1 cm, 2 cm, and 4 cm. The 1 cm region is marked TOP. The 2 cm region is marked MID, and the 4 cm region is marked BOT. Participants will use the MID section for all three trials. - Keep instructions visible during each trial.
Note: The instructions for the task are displayed at the top of the monitor and are as follows: "DH lleellee MID Normal Speed". The participant should be told prior to starting the program that these instructions mean to write the word LLeeLLee in the MID section with the dominant hand and at a comfortable handwriting speed. Also note that the software will redo trial automatically if the participant makes an error while writing.
4. Processing Trials
- Process trials using a Fast Fourier Transform Low Pass 12 Hz filter, with a 1.75 Sharpness, 1 Lump decimates sample, and 1 Up-sample Factor. Remove trailing pen lift and rotate to horizontal baseline. Set additional counter clockwise rotation when segmenting at vertical velocity to zero radians.
Note: The handwriting analysis software will automatically incorporate these processing steps if they are selected within the program options. - Summarize the absolute values of target variables LLeeLLee at two centimeters for Average Normalized Jerk (ANJ) per Trial. Collapse across trial and stroke.
Note: The ANJ is a measure of movement dysfluency. Higher ANJ indicates greater dysfluency (See Figure 2). The dysfluency measure is based on the vertical component of the jerk (in cm/sec3), i.e. the 3rd time derivative of vertical position of the pen tip. Dysfluencies are caused by sudden changes in force. The 2nd time derivative, which is acceleration, is proportional to the net muscle force (if friction is neglected). Therefore, the 3rd time derivative is proportional to the force changes. To obtain an overall measure of dysfluency the vertical jerk is squared and integrated across the duration of a stroke (unit is cm2/sec5). To make this measure independent upon the duration and the vertical size of the stroke, multiply the integral by the 5th power of stroke duration (unit is sec5) and the inverse of the vertical size squared (unit is 1/cm2). The result is therefore unitless. Normalized jerk describes the shape of the acceleration curve irrespective of width and height. Take the square root of the end result to make ANJ proportional with jerk
The ANJ of a trial is defined by the average of the normalized jerk estimates across all up and down strokes of a trial 23.
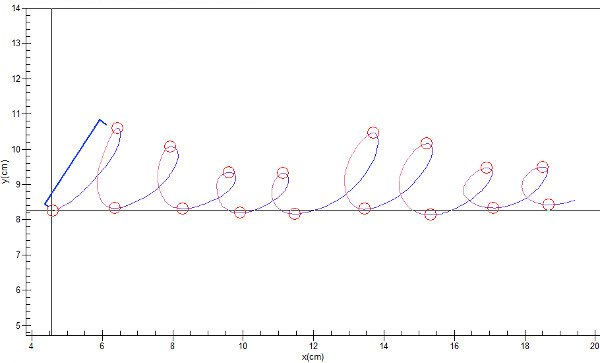
Figure 2. Trial from a control participant. Each trial is divided into 16 strokes. The segmentation of stroke for analysis of average normalize jerk is illustrated with the first pen stroke (in blue). A blue bracket outlines the stroke, and circles denote the start and stop of the stroke segment. Click here to view larger figure.
5. Statistical Analysis
- Employ independent two tailed t-tests and chi-square tests to examine differences between groups in continuous and categorical demographic variables, respectfully. If necessary, adjust for inequalities of variance by Levene's test.
- Employ an analysis of covariance (ANCOVA) controlling for nicotine use and gender with group (UHR and Control) as the independent variable and ANJ collapsed across trial.
There were no significant differences between groups on demographic characteristics including age, years of education, or parental education (see Table 1 for a demographic breakdown of the participants). Chi Square tests revealed significant differences between groups on gender χ2 (1, N = 36) = 5.46, p≤0.05, with more males in the UHR group and more females in the control group. There was a significant group differences in tobacco usage frequency, t(22.9) = 2.15, p≤0.05, showing that UHR participants smoke more than controls. UHR participants were rated significantly higher than controls on all SIPS symptom domains, including positive (t(37) = 10.9, p ≤ 0.001), negative (t(37)= 6.9, p≤0.001), disorganized (t(37) = 6.7, p≤0.001), and general (t(37) = 5.7, p≤0.001).
| UHR | Control | Total | p ≤ | |
| Age | ||||
| Mean (SD) | 18.43 (1.91) | 17.45 (2.43) | 17.97 (2.19) | 0.3 |
| Gender | ||||
| Male | 13 | 6 | 19 | |
| Female | 5 | 12 | 17 | |
| Total | 18 | 18 | 36 | |
| Race and Ethnicity | ||||
| Asian | 0 | 3 | 2 | |
| Black | 1 | 0 | 1 | |
| Hispanic | 2 | 5 | 7 | |
| White | 15 | 10 | 25 | |
| Education (years) | ||||
| Mean (SD) | 12.39 (1.85) | 11.67 (2.25) | 12.03 (2.06) | 0.3 |
| Parent Education | ||||
| Mean (SD) | 16.20 (1.57) | 15.94 (2.42) | 16.09 (2.01) | 1 |
| SIPS Positive | ||||
| Mean (SD) | 11.619 (4.33) | 0.78 (1.31) | 6.62 (6.37) | 0.001 |
| SIPS Negative | ||||
| Mean (SD) | 11.62 (6.83) | 1 (1.53) | 6.72 (7.37) | 0.001 |
| SIPS Disorganized | ||||
| Mean (SD) | 5.9 (3.56) | 0.45 (0.98) | 3.38 (3.84) | 0.001 |
| SIPS General | ||||
| Mean (SD) | 6.62 (4.26) | 0.78 (1.7) | 3.92 (4.42) | 0.001 |
| Average Normalized Jerk | ||||
| Mean (SD) | 43.92 (25.55) | 30.99 (17.29) | 36.47 (22.03) | 0.05 |
Table 1. Demographic Characteristics and Results. Demographics of the sample showed no differences in variables for age and parent education. There was a significant difference in gender between groups with more males in the ultra-high-risk group and more females in the control group.
Because tobacco use mediates the regulation of dopamine in areas responsible for movement 21,24, we examined group differences by treating frequency of tobacco use as a covariate. As gender was significantly different between groups, male/female was also treated as a statistical covariate. The groups showed a significant difference for average normalized jerk F(3, 32) = 3.98, p = 0.02, d = 0.59. These results suggest that the UHR group showed a larger value of ANJ, indicating more dysfluent pen movements (See Figure 3), and that the handwriting analysis may have detected the presence of dyskinesia in the high-risk participants.
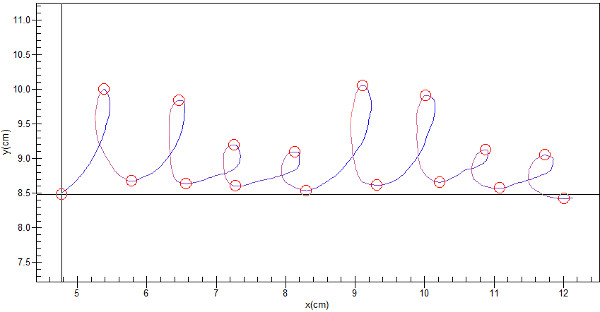
Figure 3. A UHR participant's dysfluent pen movement. Compared to a healthy control (see Figure 2), there is a significant increase in average normalized jerk for UHR participants. Click here to view larger figure.
