Manufacture of Concentrated, Lipid-based Oxygen Microbubble Emulsions by High Shear Homogenization and Serial Concentration
Summary
We describe methods for the manufacture of large volumes of lipid-based oxygen microbubbles (LOMs) designed for intravenous oxygen delivery using high-shear homogenization and serial concentration.
Abstract
Gas-filled microbubbles have been developed as ultrasound contrast and drug delivery agents. Microbubbles can be produced by processing surfactants using sonication, mechanical agitation, microfluidic devices, or homogenization. Recently, lipid-based oxygen microbubbles (LOMs) have been designed to deliver oxygen intravenously during medical emergencies, reversing life-threatening hypoxemia, and preventing subsequent organ injury, cardiac arrest, and death. We present methods for scaled-up production of highly oxygenated microbubbles using a closed-loop high-shear homogenizer. The process can produce 2 L of concentrated LOMs (90% by volume) in 90 min. Resulting bubbles have a mean diameter of ~2 μm, and a rheologic profile consistent with that of blood when diluted to 60 volume %. This technique produces LOMs in high capacity and with high oxygen purity, suggesting that this technique may be useful for translational research labs.
Introduction
Microbubbles composed of protein, polymer, and lipid shells have been developed as vectors for drug delivery, gene therapy, and ultrasound contrast agents1-5. Because these therapeutic uses require intravascular microbubble persistence, such microbubbles are commonly filled with inert, high molecular-weight gases such as perfluorocarbons6, which have low solubility in blood and stabilize the bubble3,4.
Recently, lipid-based oxygen microbubbles (LOMs) have been designed to deliver therapeutic doses of oxygen, which may preserve end-organ oxygen delivery and prevent hemodynamic instability during periods of airway obstruction or hypoxemia7. Emulsions designed for intravenous gas delivery require different design features than those used for ultrasound contrast agents or targeted drug delivery. First, because the body consumes large volumes of oxygen gas (~200 ml/min), LOMs must be produced and injected on a large scale. This requires that the manufacturing process be efficient. Second, the manufacturing process should be closed-loop in order to avoid nitrogen contamination through the exposure of LOMs (which should be filled with 100% oxygen) to ambient air. Third, because the purpose of LOMs is intravenous gas delivery, the gas fraction of LOMs should be maximized, recognizing the limitations imposed by emulsion viscosity7. Finally, as with any intravenous injectable, precise control over particle size distribution is essential to avoiding microvascular obstruction8.
There are several established methods for microbubble manufacture. Sonication utilizes high intensity, low-frequency ultrasound applied to the air-fluid interface of an emulsion which includes a surfactant, such as an amphipathic phospholipid, in the presence of a gas headspace to produce microbubbles7,9. This process is controllable by varying ultrasound frequency, power and pulse duration, and the resulting size distribution can be tailored to produce microbubbles of a specific size distribution, though sonication is rarely used in the manufacture of clinically-used microbubbles. Amalgamation is the intense mechanical agitation of a surfactant and gas in a closed system, which is also difficult to scale up to accommodate large volumes2. Droplet-based microfluidics allows precise control of microbubble size distribution10-13. Though traditionally difficult to scale up, multi-channel, high-speed microfluidics have been described which increase microbubble production efficiency13. Microbubbles manufactured using any of these methods may require post-manufacture size-reduction processes, such as centrifugal fractionation14,15 and microbubble flotation16,17.
Another established method for the manufacture of highly stable microbubbles is shear homogenization6, which can result in a stabilizing hexagonal phospholipid pattern on the microbubble surface18. Building on this concept, we describe the incorporation of an in-line high shear homogenizer to create self-assembling LOMs19. In this process, the homogenizer utilizes rapidly rotating blades in close proximity to dual fine mesh emulsor screens, creating high mechanical and hydraulic shear for the creation of microbubbles. Serial concentration of the lipid emulsion through this system yields an increasingly concentrated gas fraction, which can be even further concentrated by centrifugation.
Protocol
1. System Set-up
The system consists of a holding and concentrating tank (HCT) fitted with a single stage mixer, an in-line high shear homogenizer, a roller pump to move fluid between the HCT and the homogenizer, and a heat-exchanger (Figure 1).
- Place a sterilized, wide-mouthed 4 L glass collection vessel fitted with 2 base ports and 3 side ports beneath the single stage mixer. Lower the mixer head to the mouth of the vessel and ensure a gas-tight fitting using rubber seals or tape (in order to prevent ambient air from contaminating the head space).
- Fit one of the base ports (Figure 1, port #1) of the HCT with sterile 3/8” (ID) clear tubing, approximately 10” long, fitted with a 3-way stopcock at the tip for collection of the concentrated emulsion.
- Fit the second base port (Figure 1, port #2) with sterile 3/8” (ID) tubing, approximately 36” in length. Feed this tubing through a roller pump. Fit the inlet of the high shear homogenizer with a T-piece including two ports and connect as follows: connect tubing from port #2, through the roller pump and connect to the side port of the T-piece. Attach the other port to an oxygen tank using a low-flow oxygen gas flowmeter.
- Connect the outlet port of the high shear homogenizer to the inlet port of an in-line heat exchanger maintained at 4 °C. Connect the outlet port of the heat exchanger to the return port of the HCT (Figure 1, port #3), creating a closed loop system.
- Attach an oxygen tank (via a flowmeter) to the HCT (Figure 1, port #4). Attach a gas composition monitor that is open to atmosphere to the top port of the HCT (Figure 1, port #5).
- If sterility is desired, sterilize the glass and metal components before each use by autoclave. Sterilize the tubing components and plastic connectors by ethylene oxide before each use. This is especially important if the product is to be tested in vivo.
2. LOM Manufacture
- Place 20 g of GMP 1,2-distearoyl-sn-glycero-3-phosphocholine (DSPC) and 10 g of cholesterol in the base of the HCT. Add 1 L of Plasma-Lyte A to the HCT and hand stir for 1 min, integrating as much lipid as possible into aqueous phase.
- Lower the single stage mixer into the aqueous phase, ensuring that the entire mixer head is covered by the aqueous phase. Ensure that the top of the HCT is gas tight (see Step 1.1 above) and that there are no open side ports. Turn on the gas source attached to port #4 and wait until the oxygen fraction of the HCT headspace reaches >95%. At 10 L/min (LPM), this should take ~10 min.
- Using the single stage mixer, mix the precursor emulsion for 5 min at 5,000 rpm. The resulting mixture should appear pale white and contain no visible lipid clumps. Once mixed, unused lipid-water mixture can be stored at 4 ºC for up to 30 days before single use.
- Prime the entire closed loop system with the precursor emulsion by turning on the roller pump at 1.3 LPM. Once the system is primed, keep the pump on at 1.3 LPM.
- To begin manufacture of the LOMs, turn on the in-line high shear homogenizer to 7,500 rpm. Immediately thereafter, turn on oxygen flow to the inlet portion of the homogenizer at 0.5 LPM. Keep the single stage mixer (in the HCT) on at 3,500 rpm. LOMs are formed at the interface of rotor blades and the emulsor screens within the in-line homogenizer (Figure 2). Within minutes, fluid should become visibly more viscous. A more rigorous approach is to determine viscosity as a function of time, which can be done by removing aliquots from Port 1 during fabrication and analyzing with a viscometer.
Note: If visible air bubbles are present in the tubing exiting the mixer, oxygen flow to the in-line homogenizer is too high. Titrate down gas flow until fluid is opaque and contains no visible gas bubbles. - Run the system for 15 min, and then turn off the high shear homogenizer and the oxygen inlet to it. Continue to run the single stage mixer in the HCT until the emulsion is removed; this mitigates phase separation and keeps the product relatively uniform within the HCT.
Note: The volume of the gas-filled emulsion should increase approximately 2-3x during the serial concentration phase. If it does not, check to ensure that oxygen is flowing into the high shear homogenizer and that lipid concentrations in the precursor emulsion are correct. Efficiency of production decreases as lipid concentration decreases.
3. Collection, Concentration, Assessment, and Storage of LOMs
- Attach a sterile, modified 140 ml luer-lock syringe to the stopcock attached to base port #1 on the collection vessel. Draw up 100 ml of fluid. Tightly cap syringe and repeat until all fluid has been removed.
- Modify syringes by withdrawing 100 ml of air into the syringe and then sawing off the excess plunger and syringe material above the 140 ml mark. Fill and empty syringes using toothed forceps to draw up the plunger. This modification allows easier centrifugation.
- Centrifuge syringes with the capped end oriented downward in a refrigerated (4 ºC) bucket centrifuge at 225 x g for 10 min.
- Three layers of material will appear after centrifugation. Expel the bottom layer of excess cloudy aqueous phase and discard. The second layer is bright white and contains concentrated LOMs. Transfer concentrated foam to a gas-impermeable syringe using a three-way stopcock to prevent ambient gas contamination. Discard the final layer, which contains free oxygen gas from ruptured LOMs.
- Foam quality can be assessed by reaching ≥90% gas of concentrated foam. Calculate gas concentration as follows:
Volume % gas = [(Foam weight/ Foam volume)- 1] x 100- As a second quality control, size microbubbles by light obscuration to determine if particle size is within the expected range. It should be noted that a change in homogenization time or formulation might alter bubble size.
- Tightly cap the glass syringe with a luer-lock fitting. Concentrated LOMs can be diluted with Plasma-Lyte A at the time of use. Syringes can be stored at 22, 4, or -20 ºC; colder temperatures may provide enhanced shelf-life stability7.
Representative Results
High shear homogenization enables the efficient (i.e. within one afternoon) production of sufficient LOMs for an animal study and does not require technical expertise. Once proficient, up to 2 L of concentrated LOMs can be manufactured in 90 min.
Microbubble size and morphology was assessed by light microscopy and by light obscuration. When a 10 μl sample of LOMs was visualized, spherical LOMs were noted, as well as a relative paucity of lipid debris (Figure 3A). This is especially true when GMP product is used. When the same sample of LOMs was assessed by light obscuration, the mean particle diameter was 2.624±0.332 μm (SD). Greater than 90% of LOMs were <10 μm in diameter, and the population was polydisperse (Figure 3B).
Emulsion viscosity was heavily dependent on gas fraction (and therefore, on microbubble concentration). Two ml aliquots of LOMs of varying gas concentrations were studied using a steady state flow sweep using a 40 mm parallel plate geometry as stress was varied from 0.1 to 10,000 μN·m. All LOM gas fractions exhibit shear-thinning behavior, and this phenomenon was most pronounced at higher gas fractions. LOMs containing 60 volume % gas exhibited a rheological profile similar to blood (Figure 4A).
Finally, the oxygen content (including gas fraction and fractional concentration of oxygen) of LOMs was tested by adding varying volumes of oxygen contained within 60 volume % LOMs to aliquots of desaturated human blood with a known oxygen deficit. As previously described, the oxygen content of LOMs can be calculated from the increase in oxyhemoglobin concentration7. The relationship between volume of oxygen added within LOMs and the volumetric increase in oxygen content of the blood was 1.053±0.03025 (SD) (95% CI = 0.9865-1.120) (Figure 4B), suggesting that the LOMs tested contained nearly 100% oxygen, exhibited few trapped gas pockets (which do not efficiently transfer oxygen to blood, but float out rapidly), and effectively transfer their entire oxygen payload to human blood in vitro.
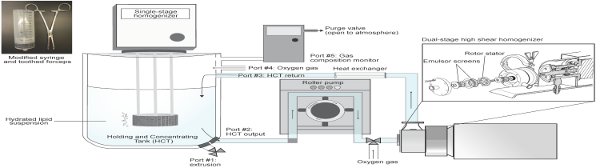
Figure 1. Manufacturing setup schematic. LOMs are produced using an in-line, high-shear homogenizer in a closed-loop system. LOMs are held within a holding and concentrating tank (HCT) under constant mixing. The emulsion is moved through the system using a roller pump. Heat generated by the homogenizer is removed using a heat exchanger. Please click here to view a larger version of this figure.
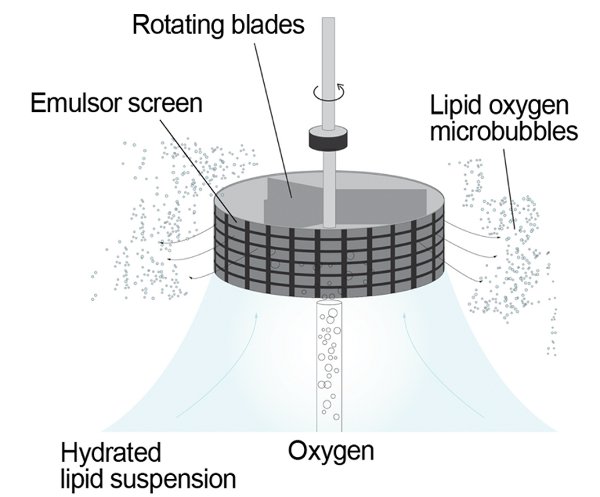
Figure 2. Self-assembly of LOMs within a fine mesh emulsor screen. A) A rapidly rotating blade passes over a fine mesh emulsor screen, creating a siphon effect that draws in the aqueous and gas phases. Tiny oxygen bubbles are formed by shear, and are quickly surrounded by the hydrophobic lipid tails of amphipathic phospholipids, creating a self-assembling gas-filled bubble (B).
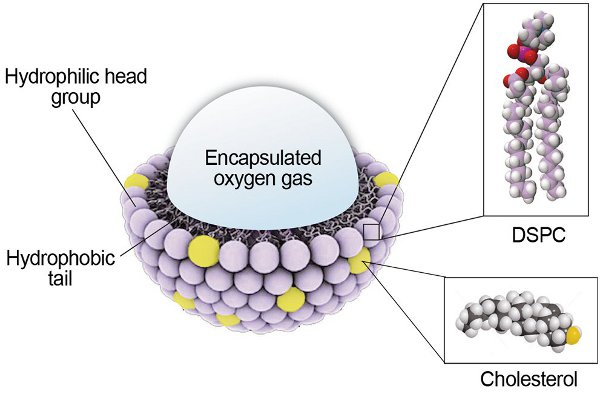
Figure 3. Characterization of LOMs. A) A representative photomicrograph of spherical LOMs exhibiting a polydisperse size distribution. Scale bar = 10 μm. B) Size distribution of LOMs as assessed by light obscuration. Data = mean, error = SEM.
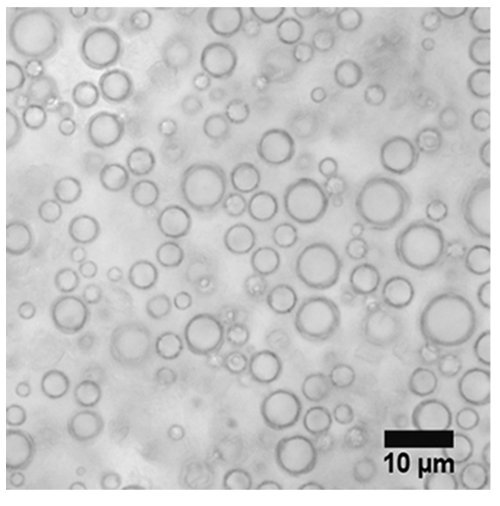
Figure 4. Properties of centrifuged and concentrated LOMs. A) The rheological profile of an LOM emulsion at 60, 70 and 90 volume % gas. Dilution of concentrated foam to 60 volume % gas yields a rheological profile similar to human blood (hematocrit 40%). Data = mean, error = SEM. B) The relationship between oxygen content of LOMs added to human blood and the measured increase in oxygen content of the blood. Data = mean, error = SEM, line = linear regression with 95% CI of the best-fit line.
Discussion
The most important steps to creating concentrated, highly oxygenated LOMs include: 1) ensuring that the headspace within the HCT remains fully oxygenated; 2) ensuring that the purity of the lipid excipients is optimal (including storage conditions and use of GMP products); 3) ensuring that the powdered lipids mix completely with the aqueous phase prior to priming the system; and 4) paying close attention to the increase in gas fraction within the HCT to ensure that the volume fraction of gas does not exceed 70%.
The method we describe here utilizes high shear homogenization to create hollow microbubbles. Amphipathic lipids are suspended with the aqueous phase, which is used to carry the lipids into the in-line homogenizer. GMP-grade lipids are utilized for in vivo studies, and are generally preferred because they contain fewer lipid aggregates and impurities. Lipids are also subject to lipid oxidation (especially when stored within an oxygenated fluid) and bacterial contamination. LOMs are formed when the hydrophobic tails arrange around small oxygen gas microbubbles created within the in-line homogenizer (Figure 2) . Homogenizing LOMs at 7,500 rpm subjects the microbubbles to additional mechanical stresses as they are milled between the tips of the rotor blades and the inner wall of the stator. LOMs also undergo hydraulic shear as they are forced at high velocity through the ultra-fine mesh emulsor screen, further reducing particle size. Shear forces generate heat within the in-line homogenizer and locally at the single stage mixer; an in-line heat exchanger before return to the HCT is necessary to remove this heat. Absence of a heat exchanger may raise temperatures above the phase transition temperature of the lipid (55 °C for DSPC), which increases the fluidity of the lipid and results in product loss. Creation of the emulsion within a closed, in-line device ensures that pure oxygen is incorporated into the LOM core by preventing air contamination. Further, LOMs are continuously exposed to with the gaseous headspace of the HCT. It is therefore imperative to ensure that the suction effect created by the lab mixer within the HCT does not create a reversal of airflow from the atmosphere into the HCT (through the gas composition monitor, which is open to atmosphere to prevent pressurization of the HCT). The oxygen gas flow rates described here should be sufficient to prevent this phenomenon.
Recycling of the emulsion through the in-line homogenizer during the serial concentration phase creates additional LOMs from ‘unused’ phospholipids remaining in the aqueous phase, and also subjects intact LOMs to repeated shearing, which may further decrease particle size. Particle size and gas concentration may be therefore tailored by adjusting mixer speeds, emulsor screens, mesh size, and run time (i.e. duration of the serial concentration step). Mechanical agitation produces a polydisperse size distribution. The wide size distribution allows for tighter packing of microbubbles, thereby increasing the maximum encapsulated gas fraction in a given volume of foam. Altering formulation chemistry by inclusion viscosity-enhancing agents may be used to create a more homogenous size distribution if desired. We have found that a run time of 15 min is most ideal; as microbubble concentration increases, the emulsion becomes increasingly viscous. Once it reaches a critical viscosity, it is no longer effectively pumped using a roller pump. This causes free gas to pass through the homogenizer without being incorporated into LOMs and can be seen within the clear tubing. At this stage, we generally elect to stop the serial concentration step, though if desired, the gas flow rate into the in-line homogenizer can be decreased and the roller pump flow rate can be increased to create higher gas fractions. However, highly viscous emulsions require more force to withdraw into syringes for the centrifugation step, and may diminish the yield of this process.
The centrifugation step has been facilitated by modifying 140 ml syringes to truncate the plunger and base of the syringe, so that filled syringes form an even cylinder. This greatly facilitates loading and unloading of syringes into the centrifuge. Following centrifugation, syringes typically contain three layers. The densest layer (near the syringe tip when syringes are loaded nose-down) contains unused phospholipids and the bulk of the aqueous phase. In some cases, cloudy ‘debris’ can be seen within the syringe tip which typically contains lipid clumps. For basic experiments, the contents of this ‘aqueous phase’ may be reused for subsequent experiments, though we have found that this substantially diminishes the efficiency of the process. (To mitigate this problem, additional phospholipid excipients may be added to the recycled precursor emulsion, taking care to maintain the molar ratio of each excipient.) The middle layer within each syringe is bright white and contains concentrated LOMs. There is typically a sharp line of demarcation between the bottom and middle layers. The middle layer of each syringe can be combined for further processing as described below. The top layer contains fluffy foam containing free gas from LOMs broken throughout the manufacturing process. The top and bottom layers are typically discarded. During centrifugation, it is important to ensure that each syringe is covered by a tight syringe cap in order to prevent the extrusion of the emulsion into the centrifuge during processing. Centrifugation at higher speeds was limited by the crush strength of the syringes we used. If needed to achieve a sharp line of demarcation between the bottom and middle layers (usually when emulsions containing high gas fraction were being centrifuged), centrifugation time can be extended. Use of a gas-tight, 3-way stopcock to combine concentrated LOMs is useful to prevent air contamination. It is also important to ensure that LOM-containing syringes are always kept capped and that any ambient air is expelled immediately. To limit air contamination during storage, syringes should be sealed with luer-lock caps only. Plastic syringes are known to be gas permeable, so glass or metal syringes are preferable for long-term storage.
As described above, emulsions exposed to the serial concentration step for 15 min typically exhibit 70% gas by volume and can be concentrated to 90% gas by centrifugation. Even if 70 volume % emulsion is desired in the end, we have found centrifugation to be helpful to remove phospholipids which are not incorporated into LOMs from the concentrate. This can also be accomplished by allowing emulsions to stand overnight to achieve phase separation. For in vivo experiments, we often dilute the concentrated LOMs with Plasma-Lyte A, mix gently, then centrifuge again to remove additional unused phospholipids and other debris. This step can be repeated several times as needed to remove excess lipid debris. The injection of phospholipids which are not incorporated into LOMs is undesirable because of the additional lipid load they impart in the setting of a high infusion rate.
We have found several common pitfalls to avoid in this manufacturing process. First, lipid excipients should be fresh, stored at -80 °C, and not used if expired. The precursor solution should not be reused for in vivo studies, as resulting emulsions are inconsistent in their size distribution and maximal gas fraction, and may contain bacterial contaminants, oxidized lipids, or lipid clumps. Second, once the emulsion reaches ‘critical viscosity’ during manufacture, it will no longer be effectively pumped through the system, and large gas pockets will form within the HCT. The high emulsion viscosity also makes the emulsion difficult to handle and draw up into syringes. These problems are best avoided by measuring the increase in gas fraction within the HCT (by quantifying the increase in volume as the gas fraction increases) and stopping the serial concentration process once the starting volume doubles.
One key limitation of this technique is the persistent need for a centrifugation step, which is undesirable because it creates the potential for air and bacterial contamination of the final product, and prevents this from being a continuous process. In the future, the serial concentration step may be modified into a single-step system for commercial drug manufacture by utilizing a hydraulic discharge system to obviate the need for batched centrifugation. The in-line homogenizer and laboratory mixers can be fabricated with 3/16 stainless steel and sterilized in place. The inclusion of other gases in the system may broaden the utility of this technique further.
Disclosures
The authors have nothing to disclose.
Acknowledgements
Funding: U.S. Army Medical Research & Materiel Command (USAMRMC) and managed by the Telemedicine & Advanced Technology Research Center. Shunxi Ji contributed the modification of the syringes as described here.
Materials
| Name of Material/ Equipment | Company | Catalog Number | Comments/Description |
| 1,2-distearoyl-sn-glycero-3-phosphocholine (DSPC) | Avanti Polar Lipids | 770365 | Alternate product: non-GMP from NOF America (Coatsome MC-8080) |
| Cholesterol | Sigma Aldrich | C75209 | |
| Plasma-Lyte A | VWR | 80089-818 | Alternatively can use NaCl |
| Glass collection vessel | Specialty Glass, Inc. | Custom | Contact: Pam Zurbrick – 281-595-2210 |
| Gas composition (oxygen) monitor | Precision Medical | PM5900L | |
| Sarns 8000 roller pump | Calicut Medical | 16407 | Part of a modular perfusion system |
| BIOtherm Heat Exchanger | Medtronic | ECMOtherm-II | |
| Verso laboratory in-line mixer | Silverson Machines, Inc | TH-IL-102-VERSO | Use multistage workheads and front-end extension with T piece |
| T-piece for Silverson Verso inlet port | Process Innovations | Custom | Contact: Brian Leavitt – 508-423-2266 |
| L5M-A laboratory mixer | Silverson Machines, Inc | NC0136483 | Use mesh emulsor screen (fine) |
| Rochester-Ochsner toothed forceps | Fisher Scientific | 13-812-18 | |
| 140 mL syringe | Kendall Healthcare Monoject | 8881114030 | Ensure there is a luer lock. |
| IX71 Inverted light microscope | Olympus | IX71 | |
| Retiga-2000R microscope camera | QImaging | RET-2000R-F-M-12 | |
| Accusizer 780A Autodilution | PSS-NICOMP Particle Sizing Systems | Out of production |
References
- Lentacker, I., De Smedt, S. C., Sanders, N. N. Drug loaded microbubble design for ultrasound triggered delivery. Soft Matter. 5 (11), 2161-2170 (2009).
- Ren, J. L., et al. A Novel Ultrasound Microbubble Carrying Gene and Tat Peptide: Preparation and Characterization. Academic Radiology. 16 (12), 1457-1465 (2009).
- Tinkov, S., et al. Microbubbles as Ultrasound Triggered Drug Carriers. Journal of Pharmaceutical Sciences. 98 (6), 1935-1961 (2009).
- Hernot, S., Klibanov, A. L. Microbubbles in ultrasound-triggered drug and gene delivery. Advanced Drug Delivery Reviews. 60 (10), 1153-1166 (2008).
- Lanza, G. M., et al. A novel site-targeted ultrasonic contrast agent with broad biomedical application. Circulation. 94 (12), 3334-3340 (1996).
- Cavalli, R., et al. Preparation and characterization of dextran nanobubbles for oxygen delivery. International Journal of Pharmaceutics. 381 (2), 160-165 (2009).
- Kheir, J. N., et al. Oxygen Gas-Filled Microparticles Provide Intravenous Oxygen Delivery. Science Translational Medicine. 4 (140), (2012).
- Lindner, J. R., et al. Microvascular rheology of definity microbubbles after intra-arterial and intravenous administration. Journal of the American Society of Echocardiography. 15 (5), 396-403 (2002).
- Zhao, Y. Z., et al. Preparation, characterization and in vivo observation of phospholipid-based gas-filled microbubbles containing hirudin. Ultrasound in Medicine and Biology. 31 (9), 1237-1243 (2005).
- Seo, M., et al. Microfluidic Assembly of Monodisperse, Nanoparticle-Incorporated Perfluorocarbon Microbubbles for Medical Imaging and Therapy. Langmuir. 26 (17), 13855-13860 (2010).
- Wan, J. D., Stone, H. A. Coated Gas Bubbles for the Continuous Synthesis of Hollow Inorganic Particles. Langmuir. 28 (1), 37-41 (2012).
- Duncanson, W. J., et al. Monodisperse Gas-Filled Microparticles from Reactions in Double Emulsions. Langmuir. 28 (17), 6742-6745 (2012).
- Kendall, M. R., et al. Scaled-Up Production of Monodisperse, Dual Layer Microbubbles Using Multi-Array Microfluidic Module for Medical Imaging and Drug Delivery. Bubble Science Engineering and Technology. 4 (1), 12-20 (2012).
- Szijjarto, C., et al. Effects of Perfluorocarbon Gases on the Size and Stability Characteristics of Phospholipid-Coated Microbubbles: Osmotic Effect versus Interfacial Film Stabilization. Langmuir. 28 (2), 1182-1189 (2012).
- Rossi, S., Waton, G., Krafft, M. P. Phospholipid-Coated Gas Bubble Engineering: Key Parameters for Size and Stability Control, as Determined by an Acoustical Method. Langmuir. 26 (3), 1649-1655 (2010).
- Swanson, E. J., et al. Phospholipid-Stabilized Microbubble Foam for Injectable Oxygen Delivery. Langmuir. 26 (20), 15726-15729 (2010).
- Kvåle, S., et al. Size fractionation of gas-filled microspheres by flotation. Separations Technology. 6 (4), 219-226 (1996).
- Dressaire, E., et al. Interfacial polygonal nanopatterning of stable microbubbles. Science. 320 (5880), 1198-1201 (2008).
- Kheir, J. N., et al. Bulk Manufacture of Concentrated Oxygen Gas-Filled Microparticles for Intravenous Oxygen Delivery. Advanced Healthcare Materials. , (2013).
