The myocardial infarction procedure occurs within 25-30 min and shows a mortality rate of 10%. After surgery, the mice recover from anesthesia within the next 15 min. No physical impairment was observed to the operated mouse. However, there is a higher risk of heart rupture one week after post-chronic myocardial infarction, if the repairing processes are disturbed during the inflammatory phase. Since heart is able to change significantly its dimensions during the pumping, it is important for all the collected hearts to be stopped in the same position, for example in diastola. This can be achieved by perfusing the heart with saturated KCl solution. Increased extracellular K+ concentration blocks the ionic pumps, decreases the membrane resting potential of cardiac cells, resulting in a diastolic arrest of cardiac activity.
The infarction area can be seen in ultrasound analysis (Figure 3A, lower panel). In comparison to the normal myocardium, ischemic regions appear thin and hypokinetic (Figure 3A, upper panel). Depending on the model used, the infarction size will differ. The chronic infarction model induces circular, transmural infarction of the apex (Figure 3B), while the ischemia/reperfusion induces a thin, middle-wall and throughout all heart (Figure 3C). There are many methods to determine infarction size. If the aim is to analyze the direct effect on cardiac viability, an Evans-Blue/TTC staining18 is indicated to be performed at least 2 hours after reperfusion, to be able to see any changes in the myocardium. Sections can be analyzed immediately (Figure 3B, middle panel) after staining or can be kept between glass slides in formalin for 2-3 days (Figure 3C, middle panel). The blue area represents the healthy myocardium, not affected by ischemia. The red area represents the viable myocardium inside the ischemic area (risk myocardium), and the white area represents the dead tissue. Usually, the infarction size is expressed as percent from the risk area.
The mature scar resulting after remodeling processes can be easily measured by immunohistolgy using Gomori's one-step staining. Blue-stained infarcted and red-stained healthy ventricular areas (Figure 3B and C, right panels) are determined in the first section from each level until the mitral valve. To avoid the variation due to binding of LAD at different levels, the infarction from all section is considered and expressed as a percentage of total left ventricular volume. An infarction volume of 15-20% in chronic infarction model and of 10-15% after ischemia/reperfusion model can be achieved. Further, the chronic infarction model will induce an accentuated dilatation, not observed in the ischemic/reperfusion model (Figure 3B and C right panel).
Conventional staining procedures can be used, such as: CD31 staining used to reveal the angiogenesis (red, Figure 4A) or smooth muscle actin staining to determine myofibroblasts (green, Figure 4B). Double fluorescence staining can also be applied to identify different target molecules in the infarction area, since the absence of cardiomyocytes gives no auto-immunofluorescence (Figure 4C).
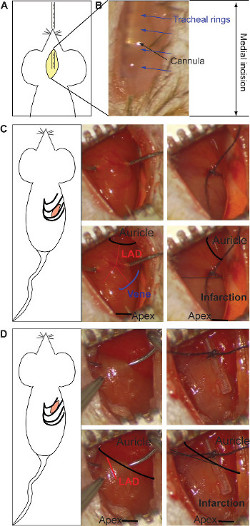
Figure 1: Medial incision and insertion of the intubation's cannula (A). The stereomicroscopic visualization of the metal cannula through the transparence of the tissue (B). The tracheal rings (blue arrows) and the cannula (black arrow) are pointed out. The intercostal incision for the chronic infarction model and the ligature of LAD (C). The ligature is located at middle of the heart (between the auricle and apex, black in lower panel), taking as reference the end of the vein (schematic in blue, lower panel). Both branches of the artery should be bound (red in lower panel). The gray color indicates infarcted area and it appears in the lower half part of the heart (right lower panel). The ligature for the ischemia/reperfusion model is made under the auricle, binding the main body of LAD (red in lower panel) over a silicon tube (right side) (D). The gray color indicates the infracted area, which is present on the entire heart (right lower panel). Please click here to view a larger version of this figure.
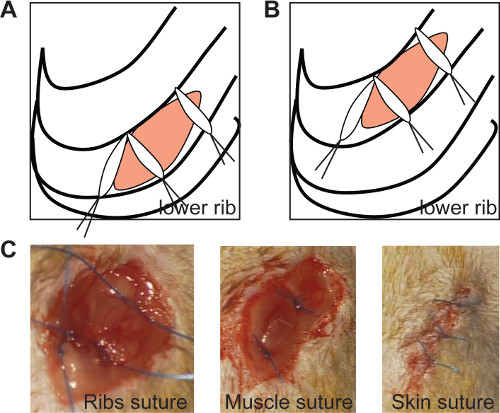
Figure 2: The ribs suture seals the thoracic incision if the medial sutures are positioned at an angle of 90° in both chronic (A) and ischemia/reperfusion model (B, left panel). In vivo imaging of ribs suture (C, left panel), muscle suture (C, middle panel) and skin suture (C, right panel). Please click here to view a larger version of this figure.
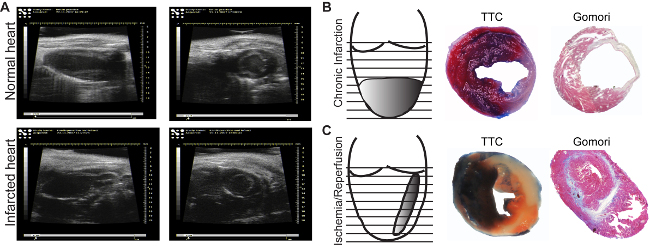
Figure 3: Echocardiographic images. Images of normal (A, upper panel) and infarcted areas (A, lower panel), are acquired in the long axis (longitudinal, left panels) or in the short axis (transversal, right panels).. Infarction induced by chronic ligature (B) and by one hr ischemia followed by reperfusion (C). Evans Blue/TTC Staining allows identification of perfused (blue)/non-perfused areas as well as the viable (red)/dead (white) myocardium (B, C, middle panels). Gomori's one-step staining allows the identification of infarcted areas (blue), and differentiates them from the normal regions (red) (B, C, right panels). Please click here to view a larger version of this figure.
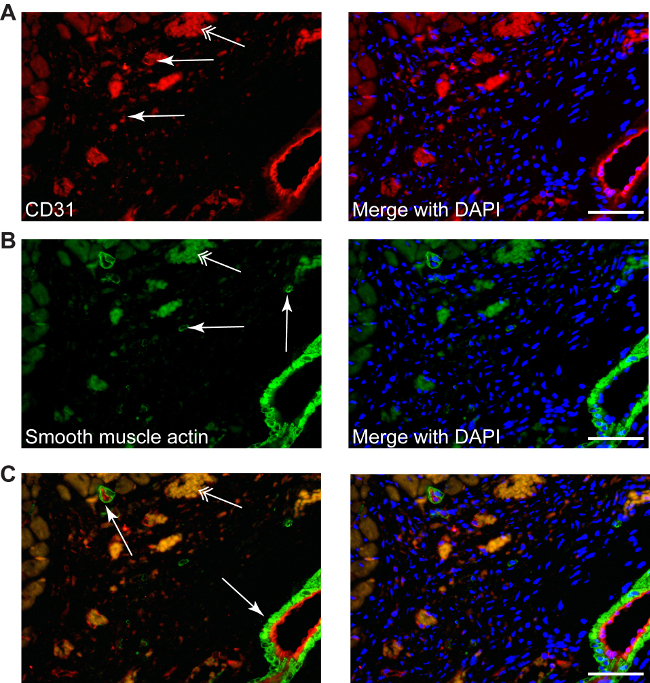
Figure 4: Different stainings can be performed in infracted area, such as CD31 to described neo-angiogenesis (A, red, simple arrows), or smooth muscle actin for myofibroblasts (B, green, simple arrows), as well as double staining (C, CD31-red/smooth muscle actin-green), counterstained with DAPI for nuclei (blue). Myofibroblasts can be differentiated easily from smooth muscle cells from small or big arteries, which are always accompanied by a endothelial layer (C, arrows). Double arrows point the erythrocytes autofluorescence. Scale bars 50 µm.
