Direct Mouse Trauma/Burn Model of Heterotopic Ossification
Summary
An Achilles tenotomy and burn injury model of heterotopic ossification allows for the reliable study of trauma induced ectopic bone formation without the application of exogenous factors.
Abstract
Heterotopic ossification (HO) is the formation of bone outside of the skeleton which forms following major trauma, burn injuries, and orthopaedic surgical procedures. The majority of animal models used to study HO rely on the application of exogenous substances, such as bone morphogenetic protein (BMP), exogenous cell constructs, or genetic mutations in BMP signaling. While these models are useful they do not accurately reproduce the inflammatory states that cause the majority of cases of HO. Here we describe a burn/tenotomy model in mice that reliably produces focused HO. This protocol involves creating a 30% total body surface area partial thickness contact burn on the dorsal skin as well as division of the Achilles tendon at its midpoint. Relying solely on traumatic injury to induce HO at a predictable location allows for time-course study of endochondral heterotopic bone formation from intrinsic physiologic processes and environment only. This method could prove instrumental in understanding the inflammatory and osteogenic pathways involved in trauma-induced HO. Furthermore, because HO develops in a predictable location and time-course in this model, it allows for research to improve early imaging strategies and treatment modalities to prevent HO formation.
Introduction
Heterotopic ossification (HO) is the formation of ectopic bone in which osteo-potent cells are aberrantly induced to form endochondral bone outside of the skeleton. While the details of the HO formation pathway are still largely unknown, an accepted paradigm includes three key factors: an inflammatory inciting incident, a permissive niche, and mesenchymal stem cells capable of forming bone.1-3 HO is a common comorbidity complicating over 60% of major burn injuries, 65% of combat-related injuries, and 10% of invasive orthopaedic surgery cases.4,5 However, it is often difficult to predict where HO will form because it can occur at sites of local injury or at distant locations that may be otherwise uninjured. This variability in location makes it difficult to intervene prophylactically to prevent reactive bone formation in a locally targeted manner. There are also congenital forms of HO such as fibrodysplasia ossificans progressiva (FOP) in which patients are prone to the development of robust HO in response to minor trauma or inflammatory insult. Powerful animal models using transgenic mice have reproduced this phenotype and provided insight to the molecular pathways that may also be important in trauma induced HO.6-9 Translational research into the pathogenesis of non-congenital HO has used a wide variety of constructs ranging from injury alone to the implantation of exogenous osteo-inductive materials and/or cells.10-13
In our prior work we have validated a simple and reliable model of HO formation in mice which does not require the administration of any exogenous material.14-17 This model created two key conditions to initiate HO: local trauma and global inflammation. This was achieved through the use of an Achilles tenotomy (local trauma) combined with a distant burn injury (global inflammation). Mice received both treatments concurrently and were found to develop a robust amount of HO that could be analyzed by histologic, radiologic, and molecular means. Interestingly, concurrent burn injury significantly increased the amount of HO that formed and accelerated its developmental time-course.14-16 HO developed at predictable sites around the calcaneus, ankle joint, and tibia/fibula of the limb that received the tenotomy. The reliability of HO development at a known location allowed for focused examination of molecular and histologic features in the early stages of ectopic ossification.14,17 To date, 100% of mice (over 50 animals) with a tenotomy and concurrent burn injury have developed HO. Additionally, longitudinal 2D and 3D imaging and spectroscopic analysis were conducted to examine the growth pattern and biochemical make-up of HO.15,16
Protocol
Ethics statement: All animal procedures were carried out in strict accordance with good animal practice as defined in the guidelines provided in the Guide for the Use and Care of Laboratory Animals: Eighth Edition from the Institute for Laboratory Animal Research (ILAR, 2011) and were approved by the Institutional Animal Care and Use Committee of the University of Michigan (PRO0001553).
1. Mouse Surgical Procedures
NOTE: Use 8-10 week old C57BL/6 mice. Other ages, backgrounds, and strains of mice can also be used to test different conditions or genetic make-up. For the tenotomy portion of the procedure, maintain sterile conditions by using face mask, hair bonnet, and sterile gown, gloves, and instruments. Surgical sites should be sterilely prepared with povidone-iodine and sterile draping. Avoid hypothermia by using a veterinary heating pad and warming resuscitation solutions to 37 °C prior to administration.
- Anesthetize the mouse using 2.5% inhaled isoflurane. Use a nose cone to leave the dorsum and hind-limbs easily accessible. Adjust the rate of isoflurane administration to maintain appropriate respiratory rate and coloration of mucous membranes and to ensure anesthesia by checking muscle tone, toe pinch, and corneal reflex. Apply bland ophthalmic ointment to the mouse’s eyes to prevent dry eye injury during the procedure. Maintain adequate body temperature using a veterinary heating pad or warm water circulator beneath the surgical field.
- Administer buprenorphine, 0.1 mg/kg, subcutaneously immediately prior to surgery for analgesia.
- Closely shave the surgical site on the left hind paw using clippers from the heel to the knee.
- Closely shave the dorsum of the mouse, beginning over the spine and extending the shaved area to the left of the dorsal midline, clearing an area at least 2 cm x 3 cm to accommodate the burn injury.
- Prepare the surgical site, including the hind paw to the knee using 3 alternating povidone-iodine scrubs.
- Perform a longitudinal incision along the medial aspect of the left Achilles tendon. Extend the incision so the Achilles tendon can be easily visualized; approximately 0.5 cm.
- Perform an Achilles tenotomy with sharp dissection of the tendon at the midpoint with sharp tissue scissors. Insert one blade of the tissue scissors in the tissue plane beneath the tendon and dissect along the plane until the blade is at the tendon midpoint. Close the scissor blades to sever the tendon sharply.
NOTE: Ensure inclusion of all posterior tendons including Gastrocnemius, Soleus, and Plantaris tendons. - Achieve hemostasis by applying pressure with sterile gauze (there should be minimal bleeding) and close the skin incision with a 5-0 vicryl stitch.
- Perform the dorsal partial thickness burn with an aluminum block weighing 35 g with approximate measurements 2 cm x 2 cm x 3 cm heated to 60 °C in a water bath applied to the shaved dorsum of the mouse for 17 sec.
NOTE: Achieve the appropriate burn depth by resting the block on top of the anesthetized mouse, ensuring that the entire surface area of the block is in contact with the mouse, however avoid applying any additional pressure to the block, i.e., allow gravity to be the only force holding the block in place. A thin plastic handle attached to one side of the block is convenient for manipulation, stabilization, and retrieval from the hot water bath. This will create an approximately 30% total body surface area burn in an 8-10 week old C57BL/6 mouse. This contact burn was chosen over other methods (flame or scald burn) due to the uniformity of burn depth over the wound and the reproducibility between animals. - Dry the burn site with gauze and apply a tegaderm dressing.
- Administer warmed resuscitation fluids: Lactated Ringer’s solution 1 ml intraperitoneal injection and 0.5 ml subcutaneous injection. This one-time administration of resuscitation is adequate for recovery from the burn injury and tenotomy.
NOTE: Do not return anesthetized mice to housing cages with other mice, house individually in clean cages under monitoring until mice are fully recovered. Typical recovery occurs within 1-6 hr. Burn sites generally heal within 2-4 weeks and are rarely complicated by wound infection if kept in clean housing environments. - Administer Buprenorphine 0.1 mg/kg subcutaneous injection every 12 hr for 3 days following the procedure. Monitor HO growth with serial µCT scans at appropriate intervals. Ectopic bone growth is first evident around 3 weeks post-op by µCT.
NOTE: The majority of HO development is complete by 9 weeks post-op. We have not observed a difference in HO volume or location with repeated µCT scans bi-weekly for 15 weeks compared to a single end-point µCT scan at 15 weeks. At the end of the experiments, euthanize all mice with CO2 inhalation according to institutional guidelines and verify death with cervical dislocation after 10 min.
2. µCT Acquisition and Analysis
- Secure the anesthetized mouse on the scanner bed in the prone position. Tape the hind limbs securely to the bed to prevent breathing motion artifact. Include the air, water, and hydroxyapatite containing phantom beneath the mouse for image calibration.
- Open the Bone Analysis software and define a region of interest (ROI) that encompasses both hind limbs from the hip joint proximally to the tip of the hind paw distally. Obtain an image using the following parameters: 80 kV, 500 µA and 1,300 msec exposure, 48 µm voxel size.14,15
- Calibrate the image to Hounsfield units (HU) by drawing a ROI in each of the three phantom chambers and inputting the average density into the appropriate fields in the software.
- Using the “grabber” tool in the software, re-orient the image so the tibia of the left hind limb is parallel along the Z axis to allow the clearest anatomical view for the delineation of orthotopic cortical bone structures and HO.
- Beginning at the knee, scroll distally through the image slices until HO is encountered. Using the manual spline tool, make an ROI around the ectopic bone on every 5th slice continuing distally through the paw or until HO has been surpassed. Use the extrapolate tool to extend and stitch the ROIs together into one ROI that contains all the HO.
- Make a 3D ROI and choose the analysis menu. Calculate the bone volume by setting the lower and upper threshold values that best show the bone window. Use the same fixed threshold values for all scans.
Representative Results
In this present study, the protocol is described for the previously published mouse model of trauma/burn induced HO.14-17 This involves the creation of concurrent localized musculoskeletal injury with an Achilles tenotomy and global inflammatory insult with a partial thickness burn injury. This results in the reliable formation of reactive bone at the tenotomy site which can be followed with serial imaging. To date, all mice (more than 50) that have sustained both Achilles tenotomy and burn injury have developed a measurable amount of HO at the tenotomy site. To quantify the formation of ectopic bone, a calibrated image µCT protocol is used at each desired time-point. The addition of a burn injury in combination with the Achilles tenotomy has proven to be key in the induction of significant HO. With both injuries happening concurrently there is a significant increase in the amount of ectopic bone that is formed at the tenotomy site compared to Achilles tenotomy alone (Figure 1).17
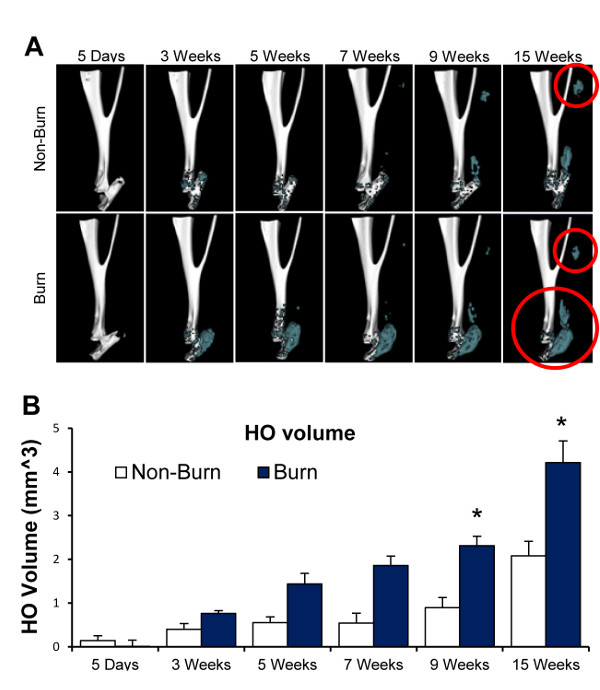
Figure 1. HO development following Achilles tenotomy with or without concurrent burn injury. All mice received an Achilles tenotomy of the left hind limb, half of the mice also received a 30% TBSA partial thickness burn injury on the dorsum. µCT scans were completed at 5 days and 3, 5, 7, 9, and 15 weeks post injury. (A). Representative 3D reconstructions are shown with orthotopic bone white and HO colored blue. Red circles indicate niduses of HO. Ectopic bone develops in the area of the tenotomy as well as locations distal and proximal to the injury site in the lower limb. Similar to HO seen clnically, this reactive bone can be contiguous with skeletal bone or develop remotely in soft tissue. (B). Quantification of HO was completed with a calibrated image protocol and shown in the graph. HO has persisted beyond 15 weeks, however development plateaus between 9-15 weeks with the greatest growth velocity typically seen between 5-9 weeks. Data are means +/- SD, n = 4 per group, Student’s t-test, *P <0.05 (Please note that this is previously published data, modified from17). Please click here to view a larger version of this figure.
Discussion
Heterotopic ossification represents a major functional impairment faced by patients that sustain trauma, burns, and invasive musculoskeletal procedures. The most at-risk population are soldiers in modern conflicts with major blast injuries from mechanisms such as improvised explosive devices (IED).18 Improved body armor and forward positioned medical units allows for improved survival of major extremity injury. After initial stabilization and repair of their extremity injury, these patients are at high risk of developing HO.18 Notwithstanding its prevalence and medical burden, relatively little is known about the details of HO development. Specifically, questions regarding the precise receptors and signaling pathways involved and the cell lineage responsible for HO are important current lines of inquiry. Some similarity to FOP and other forms of congenital HO are expected and supported by recent reports.8,14,17 A reliable model of endogenously produced HO in response to trauma is a key tool in this endeavor.
Of particular interest is the development of novel diagnostic modalities that can detect where HO is forming at early stages when preventative treatment is viable. Current treatment modalities rely on surgical excision and radiation therapy which carry significant comorbidities and high rates of recurrence.5,19,20 This is largely due the fact that HO can only be identified after it has already formed and can then be detected by conventional imaging such as radiographs or CT scans. Spectroscopic studies including near-infrared imaging and Raman spectroscopy have shown some promising preliminary results but are still in developmental phases.15,16,21
One major advantage of the mouse model described herein is the reliability and predictability of where HO will form. This factor is key in the analysis of early HO development and the preceding events that allow for reactive bone formation. Because there is no preparation or application of exogenous substances, this protocol is relatively straightforward. Critical steps include maintaining sterile technique to avoid infection of the tenotomy site, ensuring uniform contact between the aluminum block and mouse skin while creating the contact burn, and ensuring that the Gastrocnemius, Soleus, and Plantaris tendons are severed when performing the tenotomy. While one advantage of this model is its ability to induce ectopic bone in response to trauma/burn only, it is also limited by excluding other injuries that cause of HO such as fractures, traumatic brain injury, and amputations. Also, while this model has been proven to be successful in mice, it has not yet been validated in larger animals that may more accurately mimic the amount of bone that is seen in human patients.
Like all anabolic processes, ectopic bone formation is a multifactorial coordination between many different factors and players in the local environment and at the cellular level. It has been shown that HO develops in an endochondral process, however the specific precursor cell is still in question.8,14,17 Having a well-defined time-course and location of HO development is also useful in the trialing of potential preventative therapies for HO. Limiting bone morphogenetic protein (BMP) signaling or reducing inflammation following trauma/burn injuries with ATP hydrolysis have shown a significant reduction in reactive bone formation in this model.14 Further refinement and exploration of diagnostic and therapeutic modalities is certainly warranted. Key to that effort is a reliable mouse model of endogenously produced HO that mimics the processes that occur in patients that suffer the complications of HO.
Disclosures
The authors have nothing to disclose.
Acknowledgements
We thank Amanda Fair, the CMI, and Kathy Sweet and the ORL at UM for assistance with µCT imaging and analysis. Funding: BL Funded by 1K08GM109105-01 and Plastic Surgery Foundation National Endowment Award.
Materials
| C57BL/6 mice | Jackson Laboratory | 664 | 8-10 weeks old |
| Isoflurane – Fluriso | VET one, Boise, ID | V1 501017 | |
| Buprenorphine – Buprenex | Reckitt Benckiser Healthcare | NDC 12496-0757-1 | 0.3 mg/ml solution |
| Betadine | Owens and Minor, Mechanicsville, VA | 2047PVP202 | |
| 5-0 Vicryl sutures | Ethicon, Summerville, NJ | J493 | |
| Tegaderm Film, 6cm x 7cm | 3M | 1624W | Cut in half to properly cover burn site |
| µCT – GE eXplore Locus SP | GE Healthcare Pre-Clinical Imaging, London, ON, Canada | ||
| Microview 2.2 Advanced Bone Analysis Application | GE Healthcare Pre-Clinical Imaging, London, ON, Canada |
References
- Leblanc, E., et al. BMP-9-induced muscle heterotopic ossification requires changes to the skeletal muscle microenvironment. J Bone Miner Res. 26 (6), 1166-1177 (2011).
- Shore, E. M. Osteoinductive signals and heterotopic ossification. J Bone Miner Res. 26 (6), 1163-1165 (2011).
- Wosczyna, M. N., Biswas, A. A., Cogswell, C. A., Goldhamer, D. J. Multipotent progenitors resident in the skeletal muscle interstitium exhibit robust BMP-dependent osteogenic activity and mediate heterotopic ossification. J Bone Miner Res. 27 (5), 1004-1017 (2012).
- Potter, B. K., et al. Heterotopic ossification following combat-related trauma. J Bone Joint Surg Am. 92, 74-89 (2010).
- Van den Bossche, L., Vanderstraeten, G. Heterotopic ossification: a review. J Rehabil Med. 37 (3), 129-136 (2005).
- Chakkalakal, S. A., et al. An Acvr1 R206H knock-in mouse has fibrodysplasia ossificans progressiva. J Bone Miner Res. 27 (8), 1746-1756 (2012).
- Yu, P. B., et al. BMP type I receptor inhibition reduces heterotopic [corrected] ossification. Nat Med. 14 (12), 1363-1369 (2008).
- Culbert, A. L., et al. Alk2 regulates early chondrogenic fate in fibrodysplasia ossificans progressiva heterotopic endochondral ossification. Stem Cells. 32 (5), 1289-1300 (2014).
- Dinther, M., et al. ALK2 R206H mutation linked to fibrodysplasia ossificans progressiva confers constitutive activity to the BMP type I receptor and sensitizes mesenchymal cells to BMP-induced osteoblast differentiation and bone formation. J Bone Miner Res. 25 (6), 1208-1215 (1359).
- Peterson, J. R., et al. Burn injury enhances bone formation in heterotopic ossification model. Ann Surg. 259 (5), 993-998 (2014).
- Scott, M. A., et al. Brief review of models of ectopic bone formation. Stem Cells Dev. 21 (5), 655-667 (2012).
- Tannous, O., Griffith, C., O’Toole, R. V., Pellegrini, V. D. Heterotopic ossification after extremity blast amputation in a Sprague-Dawley rat animal model. J Orthop Trauma. 25 (8), 506-510 (2011).
- Tannous, O., et al. Heterotopic bone formation about the hip undergoes endochondral ossification: a rabbit model. Clin Orthop Relat Res. 471 (5), 1584-1592 (2013).
- Peterson, J. R., et al. Treatment of heterotopic ossification through remote ATP hydrolysis. Sci Transl Med. 6 (255), 255ra132 (2014).
- Peterson, J. R., et al. Early detection of burn induced heterotopic ossification using transcutaneous Raman spectroscopy. Bone. 54 (1), 28-34 (2013).
- Perosky, J. E., et al. Early detection of heterotopic ossification using near-infrared optical imaging reveals dynamic turnover and progression of mineralization following Achilles tenotomy and burn injury. J Orthop Res. 32 (11), 1416-1423 (2014).
- Peterson, J. R., et al. Effects of Aging on Osteogenic Response and Heterotopic Ossification Following Burn Injury in Mice. Stem Cells Dev. , (2014).
- Alfieri, K. A., Forsberg, J. A., Potter, B. K. Blast injuries and heterotopic ossification. Bone and Joint Research. 1 (8), 174-179 (2012).
- Hunt, J. L., Arnoldo, B. D., Kowalske, K., Helm, P., Purdue, G. F. Heterotopic ossification revisited: a 21-year surgical experience. J Burn Care Res. 27 (4), 535-540 (2006).
- Ring, D., Jupiter, J. B. Operative release of ankylosis of the elbow due to heterotopic ossification. Surgical technique. J Bone Joint Surg Am. 86-A, 2-10 (2004).
- Crane, N. J., Polfer, E., Elster, E. A., Potter, B. K., Forsberg, J. A. Raman spectroscopic analysis of combat-related heterotopic ossification. Bone. 57 (2), 335-342 (2013).
