Determining Pain Detection and Tolerance Thresholds Using an Integrated, Multi-Modal Pain Task Battery
Summary
Human pain models are valuable tools used to assess the analgesic potential of novel compounds and predict their clinical efficacy, especially when used in an integrated manner. Although implementation of these models is complex, with proper execution, the pain models described in this protocol can provide predictive and reliable results.
Abstract
Human pain models are useful in the assessing the analgesic effect of drugs, providing information about a drug's pharmacology and identify potentially suitable therapeutic populations. The need to use a comprehensive battery of pain models is highlighted by studies whereby only a single pain model, thought to relate to the clinical situation, demonstrates lack of efficacy. No single experimental model can mimic the complex nature of clinical pain. The integrated, multi-modal pain task battery presented here encompasses the electrical stimulation task, pressure stimulation task, cold pressor task, the UVB inflammatory model which includes a thermal task and a paradigm for inhibitory conditioned pain modulation. These human pain models have been tested for predicative validity and reliability both in their own right and in combination, and can be used repeatedly, quickly, in short succession, with minimum burden for the subject and with a modest quantity of equipment. This allows a drug to be fully characterized and profiled for analgesic effect which is especially useful for drugs with a novel or untested mechanism of action.
Introduction
Human pain models are useful in the evaluation of analgesics, providing information about a drug's pharmacology and identifying potentially suitable therapeutic populations. Yet the field is plagued by studies yielding inconsistent findings. The reason for these differences has been put down to the use of different pain assessment methods and different subject populations22. To correctly predict clinical analgesia, the right pain model is needed.2,13 Nevertheless, mechanism-based pain model selection has led to many failures in predicting clinical efficacy11.
The need to use a comprehensive battery of pain models is highlighted by studies whereby only a single pain model, thought to relate to the clinical situation, demonstrates lack of efficacy. No single experimental model can replicate the complex nature of clinical pain. Therefore, one pain model cannot be used exclusively to screen the pharmacological mechanism of action of a compound intended to treat clinical pain. Furthermore, the use of a panel of pain models allows a drug to be fully characterized and profiled. This is especially useful for drugs that have a novel or untested mechanism of action.
There are various paradigms for assessing validity of animal or human models of disease such as investigating the predictive, construct, concurrent or convergent, discriminant, etiological, and face validity of a model5. A pain model can be considered of higher value and more relevant to human disease the more criteria it satisfies. However, a more simple measure of validity is to evaluate a model's predictive validity and reliability6.
With early phase drug development there are also other considerations that need to be taken into account to assess the value of a pharmacodynamic measurement. The assessment should not be too burdensome, should not take too long, and the results should be quickly evaluable, automated and secure data collection is desirable. Also the ability to test several subjects concurrently requires equipment that is technically standardized and well characterized7.
While other evoked pain batteries exist, their objective is more directed towards the classification of pain and for assessing pathophysiological pain mechanisms19. Yet other batteries aim to represent a broad range of pathophysiology including pain models for muscle and visceral pain4. While suitable for testing in acute situations, their invasive nature do not make them suitable for testing repeatedly for longer periods.
The pain models presented here satisfy many of the above mentioned criteria making them especially useful for clinical studies in both healthy subjects and patients. The multi-modal pain task battery that is presented here encompasses the electrical stimulation task, pressure stimulation task, cold pressor task, UVB inflammatory model that includes a thermal task and a inhibitory conditioned pain modulation (iCPM) paradigm that takes advantage of interactions between the tasks The human pain models presented here have been tested for predicative validity and reliability both in their own right and in combination.
Protocol
Ethics statement: Procedures involving human subjects have been approved by the Stichting Beoordeling Ethiek Biomedisch Onderzoek (Foundation BEBO) and the Leiden University Medical Center.
1. Integrated Pain Assessment Tasks
NOTE: The task administration and interface is based on Spike2 software and an analogue-to-digital converter that performs the conversions needed for stimulus triggering and signal recording. This ensures uniform task administration, data capture, handling and storage, and standardizing the delivery of tasks by controlling the stimulus generation equipment while presenting instructions to the subject and feedback on slider position via a second monitor.
NOTE: Perform the tasks in short succession and in the order presented. The duration of performing all the tasks is approximately 30 min.
- Pain scoring
NOTE: For most tasks, stimuli of progressively increasing intensity are presented.- Prior to the task, present the subject with an electronic visual analog scale (eVAS) slider.
- Instruct the subject to indicate the intensity of their pain on a scale from 0 (none) to 100 (intolerable pain) by moving the slider from left to right.
- During training, and when necessary, provide the subjects with standardized definitions (Table 1) and instructions.
- Inform the subject that moving the slider all the way to the left ends the administration of the painful stimulus.
- Record when stimulus becomes painful (eVAS >0), corresponding to the pain detection threshold. Record when the pain is no longer tolerable to the subject (eVAS = 100), corresponding to the pain tolerance level of the subject and the area under the stimulus-response curve (AUC).
NOTE: During training, it is beneficial to provide subjects with a context of pain intensity. Following each task assess the maximal pain intensity using a 100 mm eVAS, with 0 and 100 defined as 'no pain' and 'worst pain imaginable', respectively (Table 1).
| Threshold | Verbal instructions to subject (during training and as a reminder) | Resulting eVAS scores |
| PDT (Pain Detection Threshold) | “Start moving the eVAS-slider when first change in sensation from non-painful to painful is felt ” | >0 ( = 1) |
| PTT (Pain Tolerance Threshold) | “When pain intensity is no longer tolerable” | 100 (intolerable pain) |
| Post-task VAS | “An example of the worst pain imaginable could be a surgical treatment without anesthetic”* | max 100 (worst imaginable pain) |
Table 1. Standard Definitions of VAS Anchor-points. *Pain is a unique personal experience; this definition is provided only to provide a consistent (nociceptive) frame of reference and is chosen as it somewhat negates experiences of loss, psychological suffering, and vicarious pain3.
2. Electrical Stimulation Task
NOTE: The task has been shown to primarily assess nociception generated from the Aδ and C sensory afferent fibers, which pass nociceptive signals from the periphery to the spinal cord. The Aδ fibers conduct the signal relatively rapidly, causing the sharp localization of pain and the rapid spinal response which is perceived during a transcutaneous electrical stimulus9. The method of electrical stimulation is based on methods described previously15.
- Clean an area of skin with skin preparation gel overlying the tibial bone, 100 mm distal from the caudal end of the patella. If required, shave the area beforehand.
- Place two Ag-AgCl electrodes on the skin. Place the middle of the first electrode (anode) 100 mm distal to the caudal end of the patella. Place the middle of the second electrode (cathode) directly (±135 mm) underneath the first.
- Record the resistance of the 2 electrodes using an ohmmeter. Ensure it is <2 kΩ. Optionally, remove the electrodes and re-cleanse the skin with skin preparation gel. Instruct the subject to sit comfortably with their foot flat on the floor.
- Connect the electrodes to a constant current stimulator and apply a tetanic pulse from 0 mA in steps of 0.5 mA/s (cutoff 50 mA), with a frequency of 10 Hz with a duration of 0.2 ms.
3. Pressure Stimulation Task
NOTE: This method of pressure pain induction has been shown to primarily assess nociception generated from the muscle with minimal contribution by cutaneous nociceptors17 and is based on methods described previously16.
- Place an 11 cm wide tourniquet cuff over the gastrocnemius muscle. Instruct the subject to sit comfortably with their foot flat on the floor. Inflate with a constant pressure rate increase of 0.5 kPa/s up to 100 kPa. Control the pressure with an electro-pneumatic regulator.
4. Cold Pressor Task
NOTE: The cold pressor task involves the submersion of an extremity (generally a hand) into cold water. It is used in clinical studies to investigate cardiovascular responses and nociception. It is also a method to induce iCPM (formerly known as diffuse noxious inhibitory control (DNIC)-like effect)18. The method of cold pressor pain is based on the methods previously described8,10.
- Prepare two thermostat-controlled, circulating water baths set at 35.0 ± 0.5 °C and 1.0 ± 0.5 °C.
- Place a 35 cm tourniquet on the subject's non-dominant upper-arm. During hand immersion, either regulate the blood pressure manually using a sphygmomanometer or by using a custom built electro-pneumatic regulator.
- Instruct the subject to sit comfortably with their palm flat, fingers spread wide without touching the bath and rate their pain intensity using the eVAS.
- Instruct the subject to place their non-dominant hand into a warm water bath for 2 min.
- At 1 min 45 sec inflate the blood pressure cuff on their upper-arm to 20 mmHg below resting diastolic blood pressure.
- At 2 min instruct the subject to move their hand from the warm water bath, directly placing their hand into the cold water bath to similar depth.
- After reaching pain tolerance, or after reaching a time limit (120 sec), instruct the subject to remove their arm from the water. At this point deflate the blood pressure cuff and give the subject a towel to dry their forearm.
5. Conditioned Pain Modulation Paradigm
NOTE: iCPM is the activation of the pain-modulatory mechanism, as part of the descending endogenous analgesia system18. The degree of iCPM is assessed by comparing the electrical pain thresholds for the single stimulus paradigm before and after the cold pressor task.
- Repeat the electrical stimulation task (section 2) within 5 min after the end of the cold pressor task.
6. Ultra-violet Inflammation Model
NOTE: The UVB "sun burn" model is a pain model in which erythema is induced on the skin by exposing the skin to UVB light in a well-controlled and reproducible manner. This exposure causes changes to the skin which leads to pain perception being intensified in the affected area (primary hyperalgesia) and is used as biomarker for inflammatory pain. This inflammation model is based on the methods previously described4. Inform subjects that the UVB exposure may leave long-lasting (6 – 12 months) skin marking/tanning and that exposure to UVB in general has been linked to premature skin aging and skin cancer.
- Determining a Subject's Minimal Erythemic Dose (MED)
- Turn on the UVB lamp and allow it to warm up for at least 10 min prior to use. Replace the fluorescent tubes once output is <3.0 mW/cm2 (after approximately 50 – 100 working hr).
- Instruct the subject to stand with their right hand holding their left shoulder. Place the UVB lamp on the right upper back / shoulder of the subject, in direct contact with the skin. Only induce the erythema on even-toned healthy skin; moles, tattoos, nevus and acne must be avoided.
- Apply the UVB exposure at the screening visit in ascending doses (see Table 2) to 6 different 1 x 1 cm areas of skin on the back to determine the individual UVB dose that produces the first clearly discernable erythema (minimal erythemic dose (MED).
- Assess the erythemic response 24 hr (±2 hr) after the exposure of the 6 doses. Determine the MED visually, by means of consensus of two observers with good color vision, by observing which dose produces the first clearly discernable erythema. Choose the 3rd UVB dose to approximate the mean MED for the respective skin type20.
| Skin type | I | II | III | IV |
| Dose | ||||
| #1 | 64 | 126 | 176 | 234 |
| #2 | 91 | 177 | 248 | 330 |
| #3 | 128 | 251 | 351 | 467 |
| #4 | 181 | 355 | 496 | 660 |
| #5 | 256 | 502 | 702 | 934 |
| #6 | 362 | 710 | 993 | 1321 |
Table 2. UVB Dose Regimen Per Skin Type ( mJ/cm2 )
- UVB exposure
- Apply a 3 x 3 cm UVB exposure equivalent to the subject's 3-fold individual MED. Apply this UVB exposure to the subject's back 24 hr prior to the first battery of tasks/dosing. Ensure the UVB exposure produces a homogeneous, well-demarcated area of skin erythema and hyperalgesia.
- Assessment of Skin Thermal Detection Threshold
- Using a 3 x 3 cm thermode measure the thermal pain detection threshold on normal skin contralateral to the site of UVB irradiation followed by UVB irradiated skin. Set the temperature initially to 34 °C, then ramp up by 0.5 °C/sec. Record the average pain detection threshold of 3 stimuli.
7. Subjects
NOTE: In addition to standard selection criteria and to ensure a reasonably homogeneous subject population the following exclusion criteria should be considered. Exclude subjects who meet the following criteria:
- Indicate nociceptive tasks are intolerable at screening.
- Achieve tolerance of >80% of maximum input intensity for cold, pressure and electrical tasks (to exclude pain tolerant individuals which may obfuscate an analgesic effect).
- Have any current, clinically significant, known medical condition, particularly any existing conditions that would affect sensitivity to cold (such as atherosclerosis, Raynaud's disease, urticaria, hypothyroidism) or pain (parasthesia, etc.). Use healthy subjects only.
- Use prescription or nonprescription drugs (especially analgesics) and dietary/herbal supplements within 7 days or 5 half-lives (whichever is longer) prior to the first dose of study treatment.
- Have dark skin (Fitzpatrick skin type V or VI), widespread acne, tattoos or scarring on back (due to interference with the UVB model).
- Sunbathe or have used sunbeds in the 6 months prior to screening or are unable to not be exposed to excessive sunlight or to sunbathe for the duration of the study. Skin coloration due to sunlight and sunburn affect the UVB study endpoints.
NOTE: Unless contraindicated, women should be included and where possible menstrual cycle should be either monitored or controlled for (e.g., testing only during luteal phase).
Representative Results
| Task | Endpoints |
| Primary Endpoints | |
| Thermal Task (Normal Skin) | PDT |
| Thermal Task (UVB Skin) | PDT |
| Electrical Task (pre-cold pressor) | PTT |
| Pressure Task | PTT |
| Cold Pressor Task | PTT |
| Secondary Endpoints | |
| Electrical Task (pre-cold pressor) | PDT, AUC, and post-task VAS |
| Pressure Task | PDT, AUC, and post-task VAS |
| Cold Pressor Task | PDT, AUC, and post-task VAS |
| Conditioned Pain Modulation Response (change from electrical pre- and post-cold pressor) | PDT, AUC, and post-task VAS |
Table 3. The Outcome Variables (Endpoints) Defined for a Study. Pain Detection Threshold (PDT), Pain Tolerance Threshold (PTT), Area Under the Visual Analogue Scale (VAS) pain Curve (AUC), and post-task VAS.
The primary outcome variable of interest is the PTT for the electrical stimuli, pressure and cold pressor tasks, and the PDT for the thermal (heat) stimuli on normal and UVB-exposed skin (Table 3). Data collected from the pain model assessments should be summarized descriptively (absolute values and change from baseline) by time and treatment. In addition, plots showing the mean (95% confidence interval (CI)) result and the mean change from baseline (95% CI) at each time point by treatment should be presented (see Figures 1 and 2). Results following placebo treatment should be relatively stable throughout the study day (Figures 1 and 2). Analgesic responses i.e., increases in the PDT or PTT, should reflect the pharmacokinetic properties of the drug. For the cold pressor task, the relatively rapid onset of action and short half-life of fentanyl and ketamine are reflected in the increase in PTT times (Figure 1). In contrast, the increase in PTT following pregabalin administration mirrors the pharmacokinetics of this drug which has a longer tmax and half-life (Figure 2). The known insensitivity of the cold pressor task for other analgesics are shown by there being little change from placebo (Figure 1 and 2). Nonetheless, the other tasks in this battery are sensitive to these drugs e.g., the UVB model captures the analgesic properties of the NSAID ibuprophen (data on file), allowing for drugs to be fully characterized.
Depending on the ultimate design of the study, analyze the endpoints with a mixed model analysis of variance (ANOVA) with treatment, time, sex, treatment by time and treatment by sex as fixed factors, with subject, subject by treatment and subject by time as random factors and with the average baseline measurement as covariate.
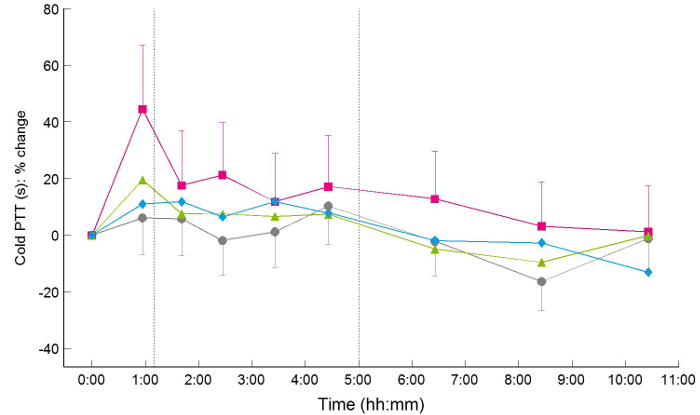
Figure 1. Effect of Intravenous Analgesics on Cold Pressor Pain Tolerance Thresholds. Example time course of the mean change from baseline profile in least square means (95% CI error bars) for the pain tolerance threshold for cold pressor task after 30 min intravenous administration of placebo (grey circle), (S)-ketamine 10 mg (green triangle), fentanyl 3 µg/kg (magenta square), and phenytoin 300 mg (blue diamond). Please click here to view a larger version of this figure.
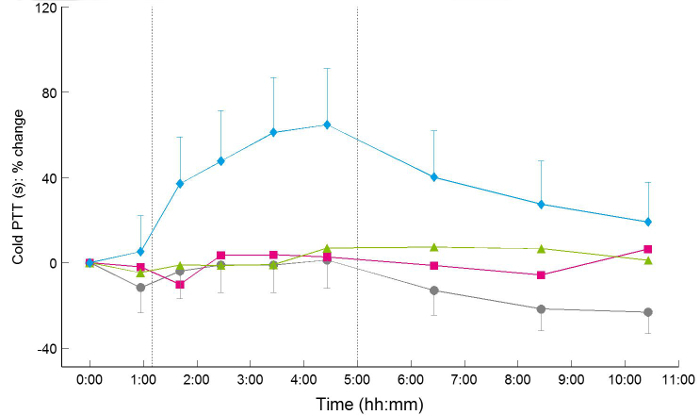
Figure 2. Effect of Oral Analgesics on Cold Pressor Pain Tolerance Thresholds. Example time course of the mean change from baseline profile in least square means (95% CI error bars) for the pain tolerance threshold for cold pressor task after oral administration of placebo (grey circle), imipramine 100 mg (green triangle), ibuprofen 600 mg (magenta square), and pregabalin 300 mg (blue diamond). Please click here to view a larger version of this figure.
Discussion
For novel and established analgesics alike, a profiling approach is proposed that utilizes reliable and predictive multi-modal pain models. In contrast to other more onerous pain tasks, such as chemical (e.g., capsaicin, nerve growth factor) hyperalgesia or visceral pain models, the pain tasks mentioned in this protocol can be used repeatedly, quickly, in short succession, with minimum burden for the subject and with a modest quantity of equipment. By using a battery of pain biomarkers such as the one mentioned in this protocol, (plasma) concentration-effect relationships can be established leading to better estimation of a drug's pharmacological activity. Thereby, more rational choices can be made regarding the therapeutic effect of a drug rather than simply using animal data and the maximum tolerated dose derived from adverse events7.
The design of a clinical study utilizing these pain models needs careful consideration. While the aforementioned pain models provide a suitable basis for screening potentially analgesic drugs, other factors need to be considered, especially taking into account the pharmacological mechanisms of the drug and its pharmacokinetics21. Standard practice for researching analgesics should be applied, including the use of positive controls and designing studies that are randomized (balanced, where applicable), placebo-controlled, and double-blind. Furthermore, it is critical that pain tasks are performed consistently between subjects, with standardized instructions and environmental conditions. While there is risk of an interaction between the tasks e.g., sensitization or additive effects, careful study design and consistent delivery of the tasks minimizes this. In fact, one of these interactions is taken advantage of in this battery by incorporating the iCPM paradigm.
When deciding to include pain tasks in a study, the overall burden of the study should be considered as this may restrict the number of treatment arms or the number of times a task is repeated. If other tasks are used, e.g., measures of sedation or alertness, this may limit the total number of tasks a subject can perform within a study day; this is especially true if populations other than healthy adult subjects are included e.g., adolescents or chronic pain patients.
A series of validated pain tasks early in drug development is crucial to bridge findings in the laboratory and those in the clinical situation, provide valuable information in regard to the mechanism of action of a new drug, choose the most applicable patient population to be studied and ascertain the most relevant nociceptive test for more intensive PK/PD modelling. PK/PD modelling can be used to identify responders and non-responders, better estimate the time-course of analgesia or aid in the development of different formulations12. By characterizing analgesics in both healthy subjects and patients, a translational connection between early phase development and the clinic can be established. It may also be used to provide information on the pain physiology and pathophysiology in these populations14. Eventually, the ability to link the efficacy profile of a drug to the pain profile of a patient could help guide individualized treatments in the future1.
Human pain models are valuable tools used to assess the analgesic potential of novel compounds and predict their clinical efficacy. While the implementation of these models can be complex and multifaceted, with proper execution, these pain models can provide predictive and reliable results.
Disclosures
The authors have nothing to disclose.
Acknowledgements
We would like to thank Esther Davidse, Michiel Weber, Rens Batist, Joop van Gerven and all other staff involved in development of these pain tasks.
Materials
| Analogue–to-digital converter | Cambridge Electronic Design (CED), Cambridge, UK | Power1401mkII | |
| eVAS slider | Cambridge Electronic Design (CED), Cambridge, UK | custom built | |
| Ag-AgCl electrodes | 3M Health Care, St Paul, Canada | Ag-AgCl Red Dot™ 2560 Electrodes | |
| Ohmmeter | Generic device | Not applicable | |
| Constant current stimulator | Cambridge Electronic Design (CED), Cambridge, UK | DS5 | |
| 11 cm wide tourniquet cuff | VBM Medizintechnik GmbH, Sulz, Germany | REF 20-90-722 | modified with Y-tube connector (REF 88404) so both chambers fill simultaneously |
| Electro-pneumatic regulator | SMC Corporation, Tokyo, Japan | ITV1030-31F2N3-Q | |
| Warm water bath & thermostat | LAUDA, Germany | Ecoline E125 | |
| Cold water bath and thermostat | LAUDA, Germany | Ecoline E212 | |
| 35 cm tourniquet | VBM Medizintechnik GmbH, Sulz, Germany | REF 20-54-711 | |
| Florescent tubes | Philips, Eindhoven, Netherlands | 36W TL01 Narrow-band | |
| 30 mm x 30 mm thermode | Medoc, Israel | TSA-II (2001) Neurosensory Analyzer | |
| Skin preparation gel | Weaver and Company | Nuprep | |
| Sphygmomanometer | Generic device | Not applicable | |
References
- Arendt-Nielsen, L. Central sensitization in humans: assessment and pharmacology. Handb.Exp Pharmacol. 227, 79-102 (2015).
- Arendt-Nielsen, L., Yarnitsky, D. Experimental and clinical applications of quantitative sensory testing applied to skin, muscles and. J Pain. 10 (6), 556-572 (2009).
- Bergh, I., Jakobsson, E., Sjostrom, B. Worst experiences of pain and conceptions of worst pain imaginable among nursing students. J Adv Nurs. 61 (5), 484-491 (2008).
- Bishop, T., Ballard, A., Holmes, H., Young, A. R., McMahon, S. B. Ultraviolet-B induced inflammation of human skin: characterisation and comparison with traditional models of hyperalgesia. Eur J Pain. 13 (5), 524-532 (2009).
- Bloom, F. E., Kupfer, D. J. . Psychopharmacology : the fourth generation of progress. , (1995).
- Bloom, F. E., Kupfer, D. J. . Neuropsychopharmacology : the fifth generation of progress. , (2002).
- Cohen, A. F., Burggraaf, J., van Gerven, J. M., Moerland, M., Groeneveld, G. J. The use of biomarkers in human pharmacology (Phase I) studies. Annu.Rev Pharmacol Toxicol. 55, 55-74 (2015).
- Eckhardt, K., et al. Same incidence of adverse drug events after codeine administration irrespective of the genetically determined differences in morphine formation. Pain. 76 (1-2), 27-33 (1998).
- Handwerker, H. O., Kobal, G. Psychophysiology of experimentally induced pain. Physiol Rev. 73 (3), 639-671 (1993).
- Jones, S. F., McQuay, H. J., Moore, R. A., Hand, C. W. Morphine and ibuprofen compared using the cold pressor test. Pain. 34 (2), 117-122 (1988).
- Lotsch, J., Oertel, B. G., Ultsch, A. Human models of pain for the prediction of clinical analgesia. Pain. 155 (10), 2014-2021 (2014).
- Martini, C., Olofsen, E., Yassen, A., Aarts, L., Dahan, A. Pharmacokinetic-pharmacodynamic modeling in acute and chronic pain: an overview of the recent literature. Expert Rev Clin Pharmacol. 4 (6), 719-728 (2011).
- Oertel, B. G., Lotsch, J. Clinical pharmacology of analgesics assessed with human experimental pain models: bridging basic and clinical research. Br J Pharmacol. 168 (3), 534-553 (2013).
- Olesen, A. E., Andresen, T., Staahl, C., Drewes, A. M. Human experimental pain models for assessing the therapeutic efficacy of analgesic drugs. Pharmacol Rev. 64 (3), 722-779 (2012).
- Olofsen, E., et al. Alfentanil and placebo analgesia: no sex differences detected in models of experimental pain. Anesthesiology. 103 (1), 130-139 (2005).
- Polianskis, R., Graven-Nielsen, T., Arendt-Nielsen, L. Computer-controlled pneumatic pressure algometry–a new technique for quantitative sensory testing. Eur.J Pain. 5 (3), 267-277 (2001).
- Polianskis, R., Graven-Nielsen, T., Arendt-Nielsen, L. Pressure-pain function in desensitized and hypersensitized muscle and skin assessed by cuff algometry. J Pain. 3 (1), 28-37 (2002).
- Pud, D., Granovsky, Y., Yarnitsky, D. The methodology of experimentally induced diffuse noxious inhibitory control (DNIC)-like effect in humans. Pain. 144 (1-2), 16-19 (2009).
- Rolke, R., et al. Quantitative sensory testing: a comprehensive protocol for clinical trials. Eur J Pain. 10 (1), 77-88 (2006).
- Sayre, R. M., Desrochers, D. L., Wilson, C. J., Marlowe, E. Skin type, minimal erythema dose (MED), and sunlight acclimatization. J Am Acad Dermatol. 5 (4), 439-443 (1981).
- Staahl, C., Olesen, A. E., Andresen, T., Arendt-Nielsen, L., Drewes, A. M. Assessing efficacy of non-opioid analgesics in experimental pain models in healthy volunteers: an updated review. Br J Clin Pharmacol. 68 (3), 322-341 (2009).
- Staahl, C., Reddy, H., Andersen, S. D., Arendt-Nielsen, L., Drewes, A. M. Multi-modal and tissue-differentiated experimental pain assessment: reproducibility of a new concept for assessment of analgesics. Basic Clin Pharmacol Toxicol. 98 (2), 201-211 (2006).
