The cadaveric femora were shipped frozen and maintained at -20 °C until preparation began. BMD scanning was performed using a DXA scanner to measure total hip and neck BMD as well as T-score for each specimen (Figure 1). A T-score is the number of standard deviations of the measured BMD compared to average values for young healthy subjects. It can range from -2.5 or lower for osteoporotic bones, between -1 and -2.5 for osteopenic bones and higher than -1 for normal bones. Once finished, bones were cleaned of excess tissue, and cut to remove the distal end using an in-house designed and fabricated cutting fixture (Figure 2). The specimens were then potted distally using a fixture designed for holding the bones in the desired internal rotation orientation; after placing the distal end into the potting container, the PMMA in liquid form was poured to fill the container (Figure 3). The X-ray images were obtained for paired bones together and for single bones separately to discern the presence of fracture or diseases, such as cancer, that might affect femoral strength (Figure 4). In the presence of such abnormalities, the condition of the bone should be documented when considered for future analyses. Finally, the femora were CT-scanned, in order to obtain CT images, using an acrylic CT scanning fixture designed to hold the bone in appropriate predetermined orientations (adduction and internal rotation angles) (Figure 5). The CT images are used to obtain 3-dimensional bone geometry and volumetric bone mineral distribution to be used in quantitative CT-based finite element analysis. Prior to subsequent fracture testing, all relevant data characterizing each femur such as the BMD values, X-ray images, and CT images were checked to ensure that data of interest were recorded and saved.
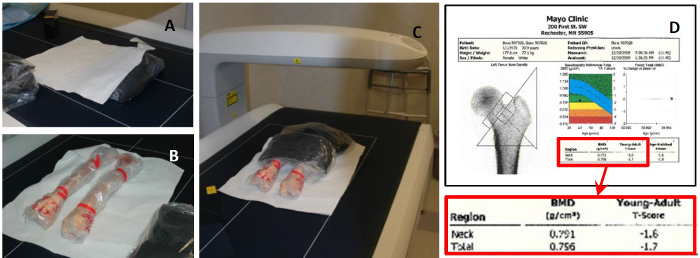
Figure 1: BMD Measurement Using DXA Scanning. (A) Rice bags and plastic lined papers; (B) Two bone specimens in desired orientations in scanner bed; (C) proximal femur ends covered with 2 rice bags during scanning; (D) Neck and total hip BMD measurements with associated T-scores. DXA scanning is performed using a clinical scanner to measure bone mineral density and estimate T-score. Please click here to view a larger version of this figure.
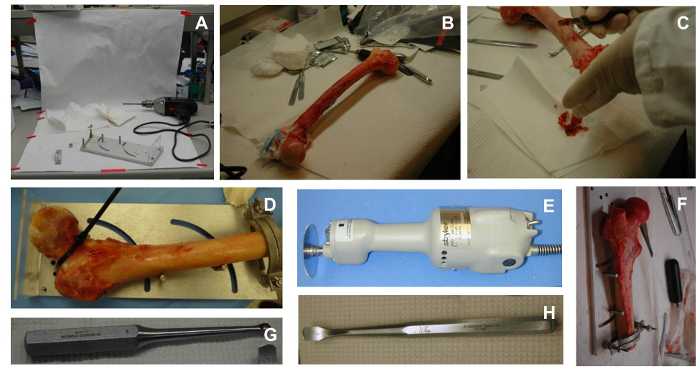
Figure 2: Cleaning and Cutting Bones. (A) Cleaning and cutting desk; (B) bone sample tools for cleaning; (C) cleaning the shaft of a femur; (D) securing a sample in the cutting fixture; (E) cast cutter; (F) completed sample after cutting. A special fixture and bone cleaning and cutting tools are used to prepare the most proximal 255 mm length for testing; (G) curette used for cleaning intramedullary canal of the femur; (H) tool for cleaning superficial tissue in samples. Please click here to view a larger version of this figure.
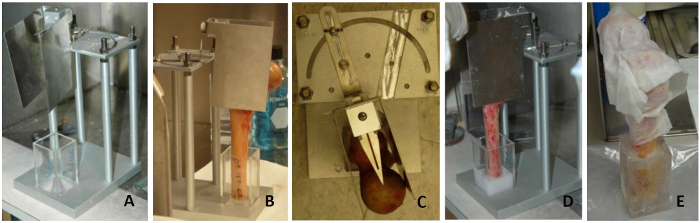
Figure 3: Femur Cleaning and Potting Process. (A) Potting fixture; (B) potting a femur in the fixture; (C) adjusting internal rotation angle to desired value; (D) pouring PMMA in the container; (E) potted bone wrapped in a saline saturated towels. A special fixture is used to set the internal rotation angle to a specified value. Please click here to view a larger version of this figure.
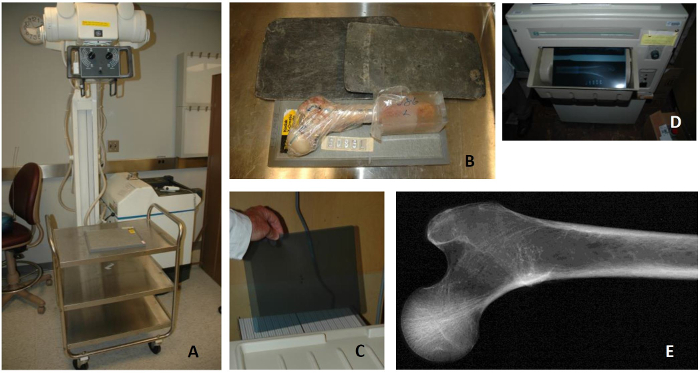
Figure 4: Bone X-ray Process. (A) X-ray machine; (B) bone sample on a cassette with unexposed film, a second half of the cassette is covered by lead to avoid exposure of the entire film; (C) placing unexposed film in loading tray of developer in dark room; (D) developed film; (E) resulting X-ray image of a healthy femur. X-ray equipment is used to scan the bones in two positions to rule out prior fractures, implants, bone metastasis, or any structural abnormalities. Please click here to view a larger version of this figure.
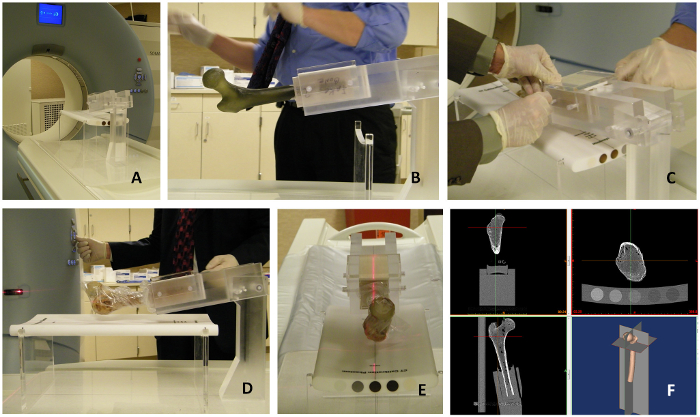
Figure 5: CT Scanning Using an Acrylic Fixture to Hold Bones in a Desired Orientation. (A) CT scanner; (B) fiberglass femur mounted in an acrylic fixture designed to hold bones in a desired orientation; (C) mounting a cadaveric femur in the fixture; (D) vertical alignment of the fixture using the CT long axis laser; (E) Alignment of the femur. An in-house designed fixture is used to hold the bone in a position identical to the subsequent testing position; bone alignment is obtained with the aid of the CT built-in lasers; (F) CT imaging of the femur. Trabecular and cortical bone can be visualized in the CT image. Cortical bone is represented by bright voxels (large Hounsfield Unit (HU) values) surrounding the trabecular bone which is represented by smaller HU values. Note: Care has to be taken to include all five rods and the entire proximal femur in the CT images. Please click here to view a larger version of this figure.
