In developing this new model, we observed many advantages in utilizing hairless SKH-1 over C57BL/6J mice, which we have used in the past. Animals subjected to STZ injections normally experience gradual weight loss with the onset of diabetes; however, in wound healing experiments previously conducted by our laboratories reproducing the model presented by Dunn et al. (2012)9 using C57BL/6J, drastic weight loss was observed (Figure 1). In contrast, when using this wound model with SKH-1 mice a statistically significant lower weight loss was observed (P<0.0001, Mann-Whitney U test). Furthermore, no deaths occurred in the diabetic SKH-1 mice cohort infected with P. aeruginosa Xen 41 biofilms while a 40% mortality rate was observed for C57BL/6J infected mice in previous experiments (Figure 2).
Another advantage to the model presented here is that the experimental procedure for the hair removal step mandatory for C57BL/6J mice is unnecessary for SKH-1 mice. Although in our previous experiments with haired mice special attention was given to minimize irritation to the skin, some damage inevitably occurred (Figure 3). Notably, however, the greatest advantage in utilizing hairless mice in this model is the elimination of the problem of hair re-growth observed in long term wound healing studies. In our experience with C57BL/6J mice, hair re-growth varied from animal to animal but given the long-term nature of the studies, it always occurred and interfered with wound area measurements or dislocated wound splints and/or dressings used to cover infected wounds, potentially resulting in drying of the wound (Figure 4).
In the SKH-1 wound healing model, after diabetes is confirmed, surgery can easily be executed to create a circular full-thickness wound on the back of the animal. The silicone splint is kept in place by a medical waterproof skin adhesive and avoids direct contact from the occlusive dressing with the newly created wound bed (Figure 5).
P. aeruginosa Xen 41 bioluminescent biofilms grown on polycarbonate membranes (Figure 6) are easily and aseptically transferred to a syringe to be prepared for delivery to the wounds and the inoculated mice are monitored daily for clinical signs of infection (Figure 7). For this model, we implemented two distinct phases. In the first phase, after inoculation of the biofilm the wound was surrounded by a splint covered with a transparent occlusive dressing. This results in pus accumulation that occluded the wound. Biofilm-containing wounds were imaged daily with the in vivo imaging system to monitor infection development and assess biofilm evolution (Figure 8 and Figure 9). Bioluminescence, recorded as total flux (p/s), can be correlated with bacterial density using a standard curve (Figure 10).
At day 8, the splint and dressing were removed to allow visualization of wound healing. Bioluminescence subsequently drops due to the loss of the pus surrounding the wound; however, bacteria remained associated with the wound as determined by histology. This approach of removing the dressing to measure wound healing has been utilized in other chronic wounds healing studies (REFs). Wound healing progression can be determined by taking micrographs with a camera attached to a microscope (Figure 11).
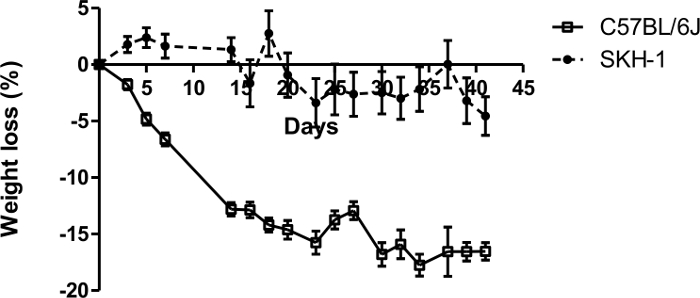
Figure 1: Comparative percentage weight loss of SKH-1 and C57BL/6J diabetic mice. Day zero corresponds to weight at the day of last (5th) STZ injection. n = 10 mice for SKH-1 and n = 12 mice for C57BL/6J. Please click here to view a larger version of this figure.
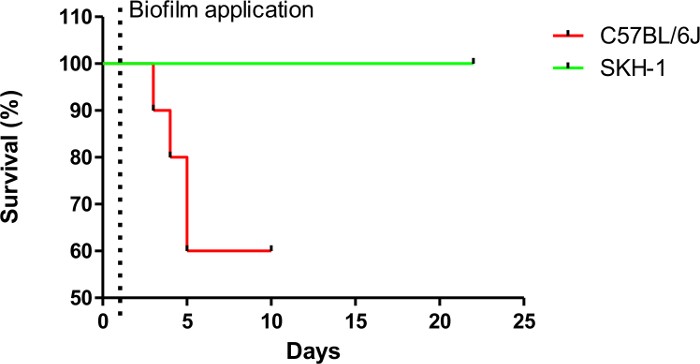
Figure 2: Percent survival rates of SKH-1 and C57BL/6J diabetic mice after P. aeruginosa Xen 41 biofilm application (day 1). n = 5 mice for SKH-1 and n = 10 mice for C57BL/6J. Please click here to view a larger version of this figure.
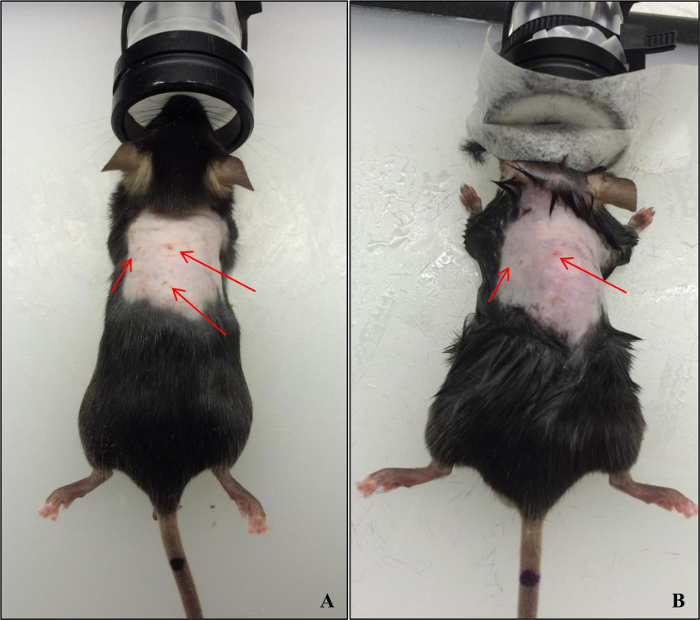
Figure 3: Skin lacerations in the future wounded area after shaving and using depilatory cream on C57BL/6J mice. (A): day of procedure; (B): 4 days after procedure. Please click here to view a larger version of this figure.
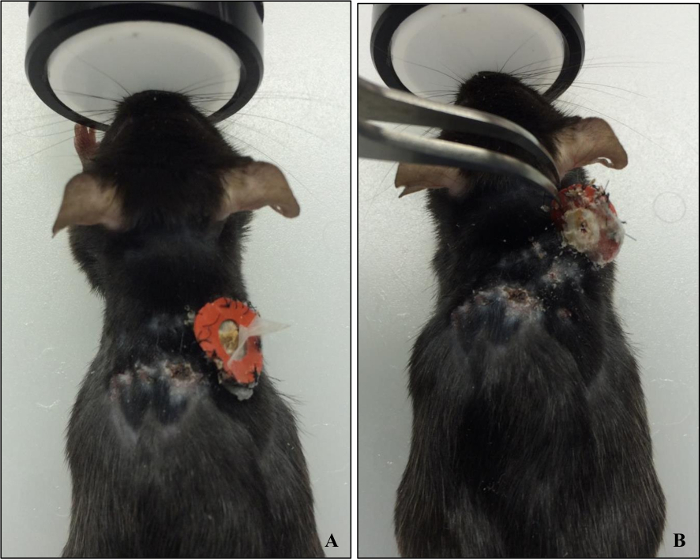
Figure 4: (A) C57BL/6J mouse with a partially removed wound splint. (B) Lifting of the splint revealed a healed wound surrounded by fully re-grown hair. Please click here to view a larger version of this figure.
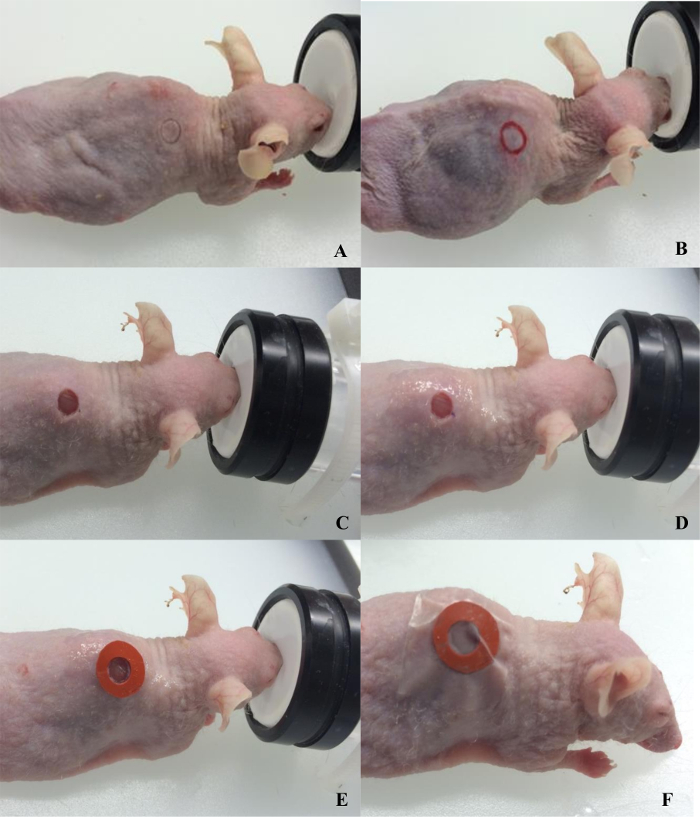
Figure 5: Surgical procedure for wounding SKH-1 mice. (A) demarcation with biopsy punch; (B) outline of the demarcation; (C) wounding completed; (D) application of medical waterproof skin adhesive; (E) glueing splint; (F) wound covered with occlusive dressing. Please click here to view a larger version of this figure.
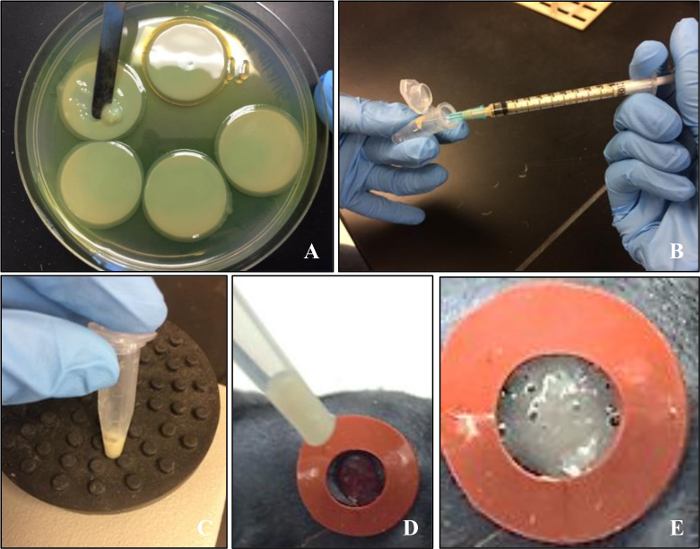
Figure 6: Preparation of the biofilm inoculum. (A) 72 h colony biofilms of Pseudomonas aeruginosa Xen 41 grown on polycarbonate membranes; (B) measurement of biofilm using a syringe. Please click here to view a larger version of this figure.

Figure 7: SKH-1 diabetic mouse 6 days after wound was inoculated with the P. aeruginosa Xen 41 biofilm. Please click here to view a larger version of this figure.
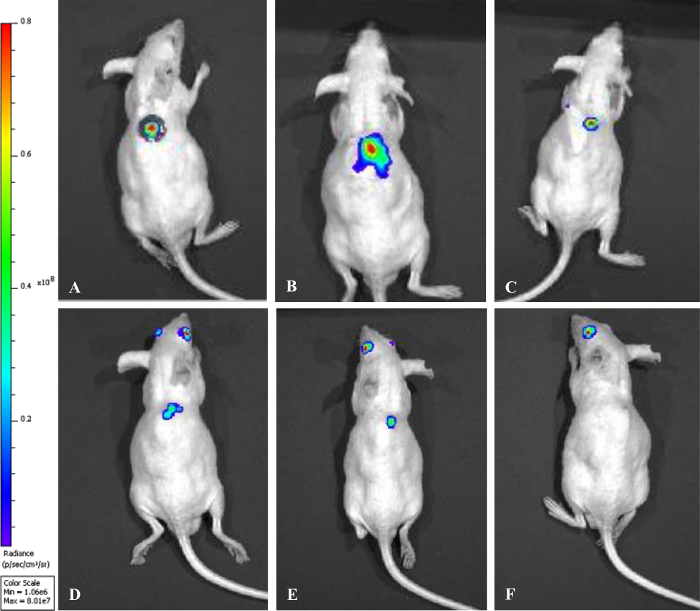
Figure 8: Monitoring of biofilm infection by tracking bioluminescence evolution over time in diabetic SKH-1 mice. (A) day of biofilm application; (B) 5 days post-biofilm; (C) 8 days post-biofilm; (D) 12 days post-biofilm; (E) 16 days post-biofilm; (F) 20 days post-biofilm. Please click here to view a larger version of this figure.
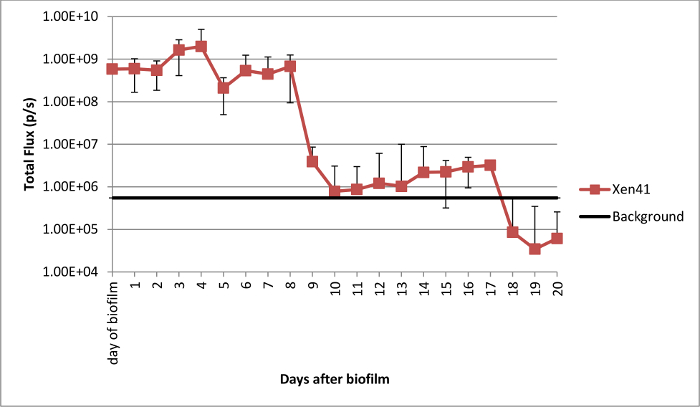
Figure 9: Total flux from wounds in SKH-1 diabetic mice infected with P. aeruginosa Xen 41 biofilms during the course of the experiment. Please click here to view a larger version of this figure.
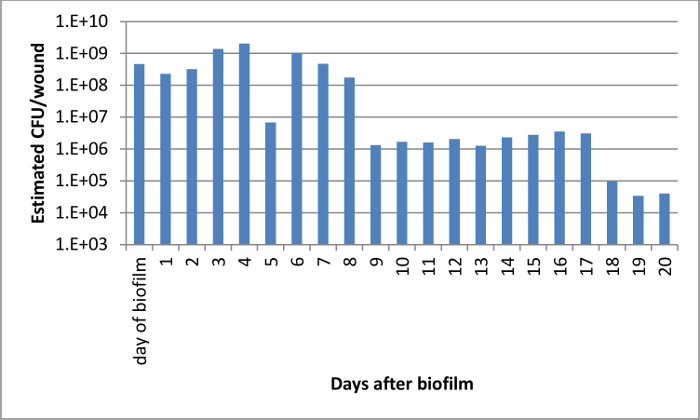
Figure 10: Estimated CFU per wound using a standard curve of bioluminescence per CFU produced with P. aeruginosa Xen 41 biofilms. Please click here to view a larger version of this figure.
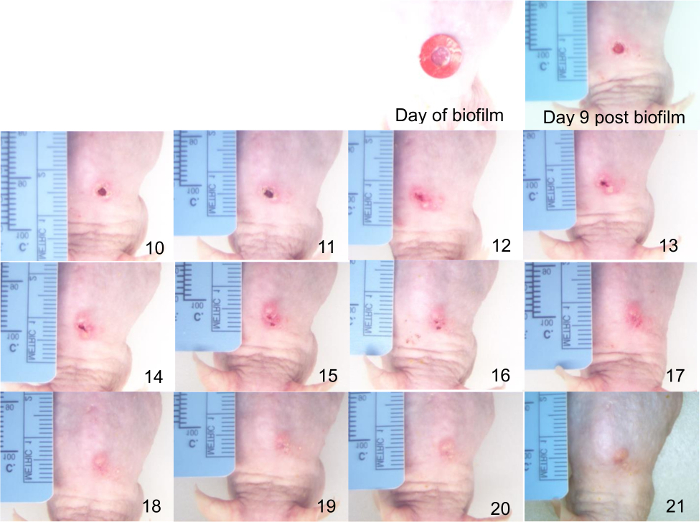
Figure 11: Micrograph timeline of wounds infected with P. aeruginosa Xen 41 biofilms in diabetic SKH-1 mouse showing progression of healing. The days after biofilm infection are indicated in the bottom left corner of each picture. Please click here to view a larger version of this figure.
