The streamlined management of patients with acute ischemic stroke as described above and shown in Figure 1 was accompanied by an improvement of peri-procedural times in our hospital. The median time from hospital admission to groin puncture was reduced by approximately half an hour when comparing the year prior to the year after implementation of the first version of the SOP (94 min in 2013 and 65 min in 2014). The revision of the SOP including the one stop management approach implemented in 2016 led to a further reduction of the median time from admission to groin puncture (65 min in 2014 and 45 min in 2016; Figure 2). The comparison of those patients who underwent EVT managed with the one stop approach (Scenario A) to those who were treated endovascularly after the initial approach, including conventional CT imaging (similar to Scenario B), shows that the median time from admission to groin puncture was reduced by slightly more than half if patients were transferred to the angiography suite directly (20.5 min in Scenario A and 54.5 min in Scenario B, Table 1). Also, the total time from hospital admission to reperfusion was significantly shorter when the one stop management approach was applied (65 min in Scenario A and 106 min in Scenario B, Table 1).
As expected, the SOP had no effect on the time from symptom onset to hospital admission (77 min before and 80 min after implementation of the SOP), as the treating stroke team cannot influence this period. The achieved times for individual steps between admission to the hospital and reperfusion before and after the SOP came into effect have been analyzed and compared (Figure 2). The faster supply of imaging (mean time between admission and imaging 31 min prior to, 19 min after the initial, and 9.5 min after the revised SOP) and in particular the prompt transfer of patients eligible for EVT to the angiography suite contributed most to the time-to-treatment reduction observed after implementation of the initial as well as the revised version of the SOP (Figure 2). The duration of EVT itself was also shorter after introduction of the initial SOP in 2014 (median 58 min prior to, and 42 min after the implementation of the initial SOP). This was independent from the devices used during EVT8. The time from groin puncture to reperfusion did not change after the revised SOP came into effect (Figure 2). The functional outcome of patients was significantly better after implementation of the first version of the SOP in 2014 (data have been published in detail elsewhere)8. Both an increase of patients with no residual functional impairment, determined by having a value of 0 on the modified Ranking Scale (mRS) (1.5% before and 9.1% after the SOP), and a general shift towards lower degrees of remaining disability was observed after workflow optimization (ordered logistic regression analysis: OR 0.56; 95% CI 0.32-0.98; p = 0.038)8.
Even though a NIHSS score of 7 points or above provides a gross estimate of the presence of LVO10, the symptoms of the patient could clearly originate from other pathologies. An observational analysis of the first 30 patients managed with the described one stop approach provides an indication of the frequency of findings other than ischemic stroke due to LVO on FDCT and FDCTA. An intracranial hemorrhage was detected in 13% (4/30) of patients and an occlusion of a peripheral vessel in 7% (2/30) of patients. Another 13% (4/30) of patients showed neither hemorrhage, vessel occlusion, nor other pathologies, and were diagnosed with Todd's paresis15.
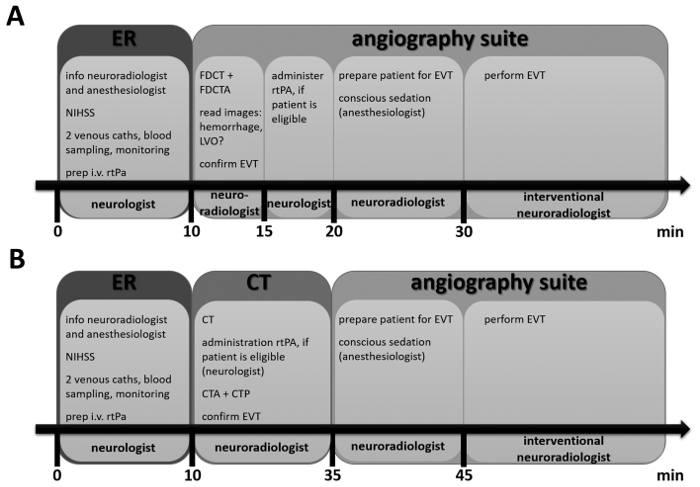
Figure 1: Timeline for Scenario A and for Scenario B. These timelines provide an overview of the steps that are performed, when a patient with suspected acute stroke is admitted to the hospital. The locations are indicated by larger boxes and the person with main responsibility for each step is indicated at the bottom. The smaller inserted boxes list actions important in each step. Details can be found in the protocol. Please click here to view a larger version of this figure.
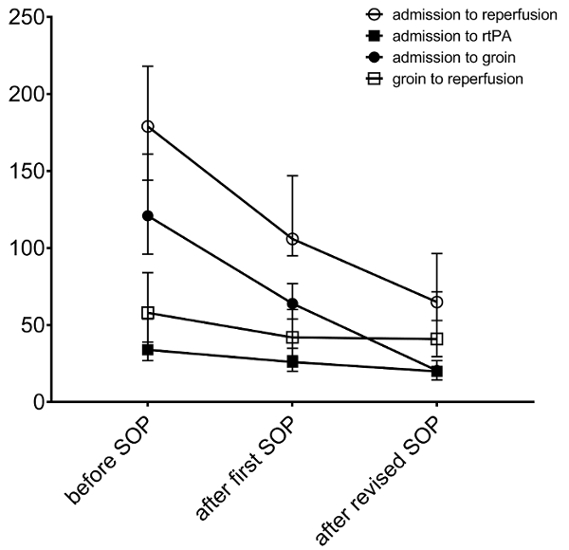
Figure 2: Representative peri-procedural times achieved with process optimization. Median times (in min) for individual steps between symptom onset and reperfusion before and after introduction of the initial as well as the revised SOP are shown. The error bars represent interquartile ranges. Please click here to view a larger version of this figure.
| door to groin (min) | door to reperfusion (min) | |||
| one stop approach (Scenario A) | conventional approach (similar to Scenario B) | one stop approach (Scenario A) | conventional approach (similar to Scenario B) | |
| n | 30 | 44 | 30 | 44 |
| Median | 20.5 | 54.5 | 65 | 106 |
| IQR | 17–27 | 44–66 | 53–96.5 | 88.5–121.5 |
| p-value | <0.001 | <0.001 | ||
Table 1: Median time from hospital admission to groin puncture and reperfusion in 2016. Scenario A consists of a one stop management approach where eligible patients (severe symptoms as determined with an NIHSS score of 7 and above and admitted to the hospital within 6 h of symptom onset) are directly transferred to the angiography suite. Imaging and EVT are performed in the same place. These patients were compared to otherwise matched (regarding NIHSS, symptom-to-door time, availability of the angiography suite) patients that were managed following the workflow implemented with the first version of the SOP. This management was similar to Scenario B and included diagnostic imaging with non-enhanced CT, CTA, and CTP. IQR, interquartile range. Statistical significance was tested with a Mann-Whitney-U test and significance level was set to α = 0.05.
