A sample size of three rats per group was used. ALT was measured at 0, 30, 60, 90, 120, 150, 180, 210, and 240 min of perfusion. We used Student's t-tests to compare results between the base perfusate and base perfusate plus PEG-CAT groups at each time point. In comparing the base perfusate and base perfusate plus PEG-CAT groups, there is significantly less (p <0.05) ALT in the base perfusate plus PEG-CAT group at 150, 180, 210, and 240 min (Figure 14A).
Liver tissue was procured in order to analyze tissue damage from both the base perfusate and base perfusate plus PEG-CAT groups. We used Student's t-tests to compare results between the base perfusate and base perfusate plus PEG-CAT groups. Tissue ATP was maintained in the base perfusate plus PEG-CAT group in comparison to the base perfusate alone group (Figure 14B, p <0.05). Tissue MDA production was significantly higher in the base perfusate group than in the base perfusate plus PEG-CAT group (Figure 14C, p <0.05). Total GSH was maintained in the base perfusate plus PEG-CAT group in comparison to the base perfusate alone group (Figure 14D, p <0.05).
To analyze apoptosis, liver tissue caspase 3/7 activity was compared between the groups. Fluorescence was measured in each well. We used Student's t-tests to compare results between the base perfusate and base perfusate plus PEG-CAT groups. Caspase 3/7 activity was significantly decreased in the base perfusate plus PEG-CAT group in comparison to the base perfusate alone group (Figure 15A, p <0.05). Terminal deoxynucleotidyl transferase (TdT) dUTP Nick-End Labeling (TUNEL) staining was used to compare apoptosis between the groups. The percentage of apoptotic cells was significantly less in the base perfusate plus PEG-CAT group in comparison to base perfusate alone group (Figure 15B, p <0.05).
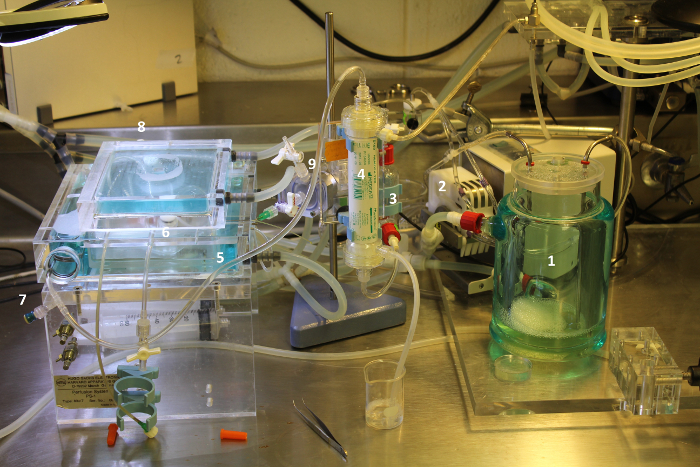
Figure 1: Perfusion Circuit. Components of the circuit are labeled. The perfusate starts in the perfusate reservoir (1), which is a water jacketed container. Perfusate is pulled from the reservoir by a roller pump (2) and pushed into a windkessel (3) and then the oxygenator (4). The oxygenator is set for countercurrent gas and perfusate flow to provide maximum gas exchange. The perfusate then proceeds to a heating coil (5) inside the perfusion chamber to ensure it is at physiologic temperature, and a bubble trap (6) to prevent perfusion of air bubbles. There are pre-organ (7) and post-organ (8) sample ports, which allow the perfusate to be sampled. The perfusate then enters the liver through the portal vein cannula. The portal vein cannula is attached to a pressure monitor, which regulates the pressure equalizer (9). Finally, the perfusate is pulled from the pressure block back through the roller pump and emptied into the reservoir. Please click here to view a larger version of this figure.
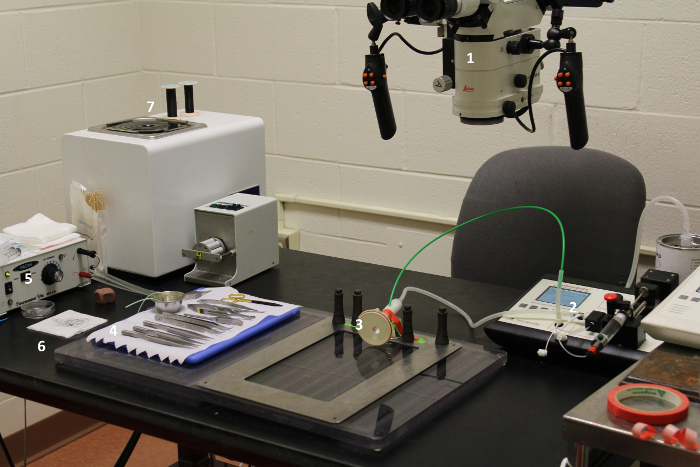
Figure 2: Operating room and surgical instrument set-up. The surgical microscope (1) should be adjusted to the appropriate height and magnification for the user. Isoflurane can be pre-loaded into the anesthesia machine (2). The animal's nose is placed in the nose cone (3). Surgical instruments should be laid out where they can be easily accessed (4). Having electrocautery (5) nearby is helpful. Sutures (6) should be pre-cut so pieces can be obtained quickly when needed, and extra should be available (7). Please click here to view a larger version of this figure.

Figure 3: Prepare the 16 G portal vein cuff. Begin with a 16 G angiocatheter. Cut a 7 mm section of tubing. Determine the midpoint of the 7 mm section by measuring 3.5 mm. Incise here and remove the anterior half of the tubing. Use a hemostat to crush this now flat portion. Use a lighter to burn the other end of the angiocatheter to create a lip. Do not place the tip directly into the flame or it will ignite. Please click here to view a larger version of this figure.
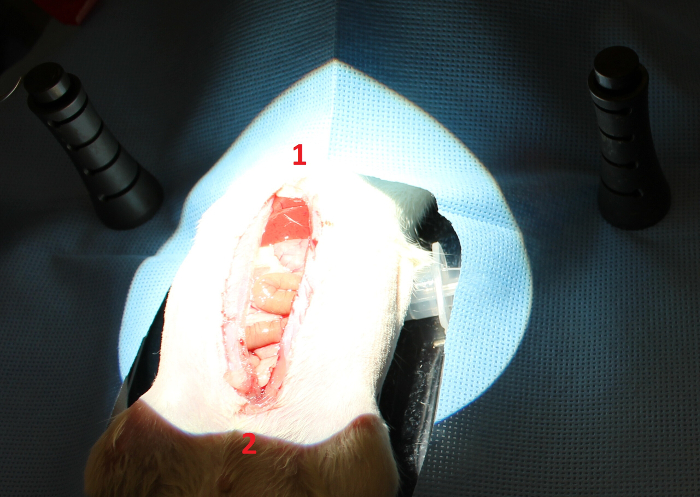
Figure 4: Midline incision. Make a midline incision from the xiphoid (1) to the pubis (2) using sharp scissors and extending through the skin and muscle. Please click here to view a larger version of this figure.
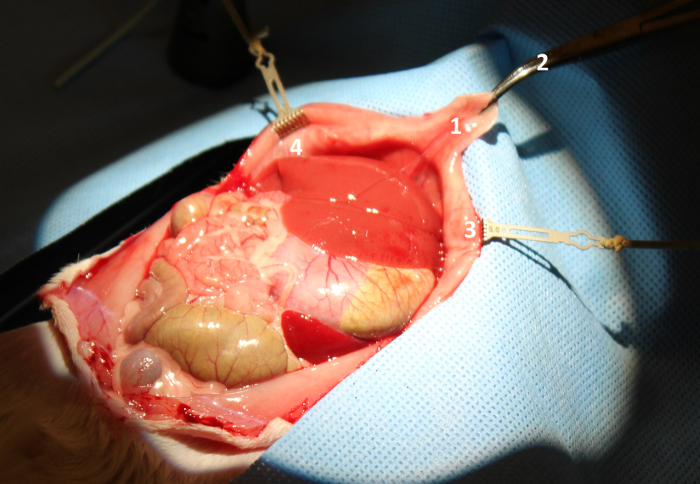
Figure 5: Obtain adequate retraction. Retract the xiphoid process (1) using a curved mosquito clamp (2) and the rib by placing rib retractors (3, 4). Please click here to view a larger version of this figure.
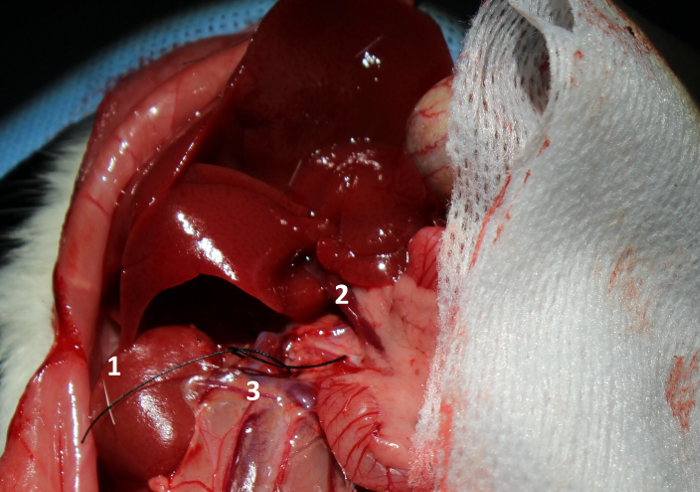
Figure 6: Inferior vena cava (IVC) dissection. Flip the liver up to expose the right kidney (1) and portal vein (2). Dissect around the IVC (3) and place a loop of 7-0 suture for future use. Please click here to view a larger version of this figure.
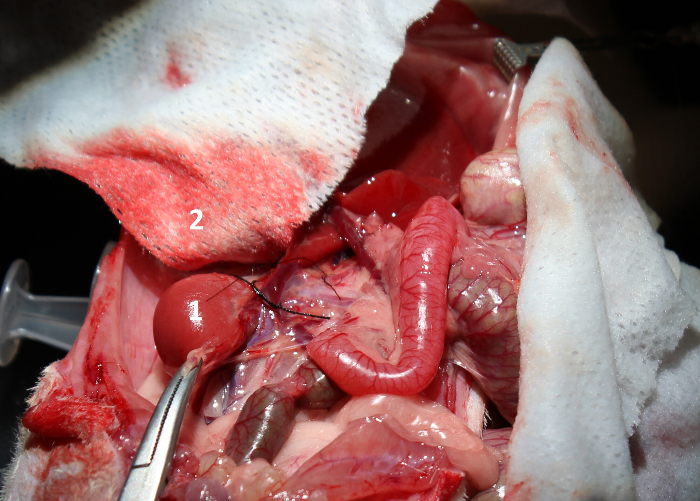
Figure 7: Ligation of the right adrenal vein. Retract the right kidney (1) to provide exposure to the right adrenal vein. Tie off the right adrenal vein and cut across it. A moistened gauze (2) can be used to protect the liver during this maneuver. Please click here to view a larger version of this figure.

Figure 8: Hepatic artery dissection. Dissect around and place a tie around the hepatic artery (1) near where it passes under the portal vein (2). Please click here to view a larger version of this figure.
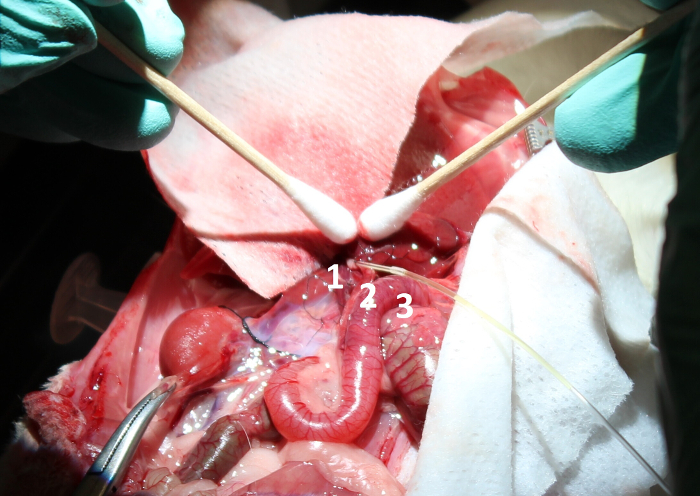
Figure 9: Bile duct cannulation. Cannulate the bile duct (1) using the 27 G angiocatheter (2) connected to the 27 G tubing (3). This will help to collect the bile during perfusion. Please click here to view a larger version of this figure.
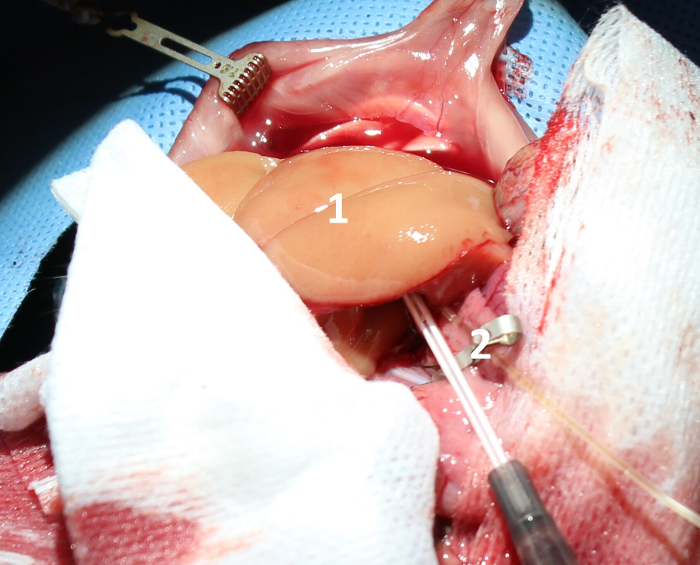
Figure 10: Liver flush. Flush the liver (1) with 60 cc of cold 0.9% normal saline with 100 U (1 mL) of heparin using a 16 G angiocatheter (2). Please click here to view a larger version of this figure.

Figure 11: After the hepatectomy. Perform a hepatectomy and place the liver in cold saline. Take care not to dislodge the bile duct cannula. Please click here to view a larger version of this figure.
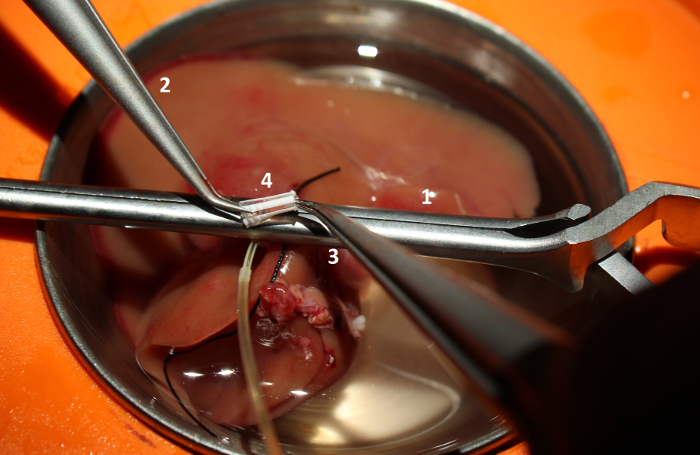
Figure 12: Portal vein cuffing. Locate the portal vein. Use a large clamp (1) to hold up the vein leaving a several millimeter-lip of vein above the clamp. Use microsurgical forceps (2, 3) to place a 16 G vascular cuff (4) in the portal vein. Please click here to view a larger version of this figure.
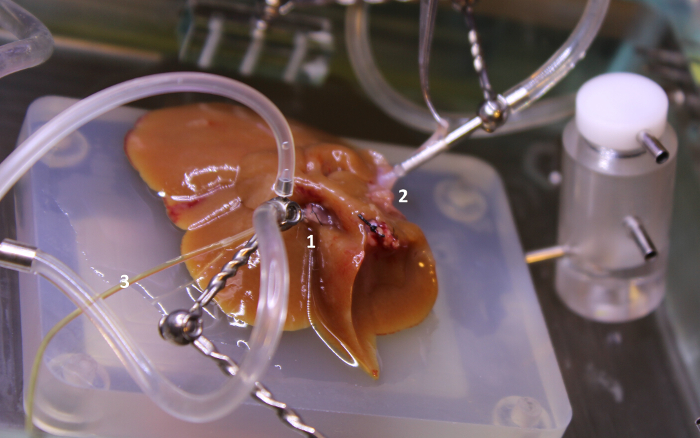
Figure 13: Portal vein cuff and superior IVC cannulation. Cannulate the portal vein cuff (1) and superior IVC (2). Great care must be taken not to dislodge the bile duct cannula (3). Additionally, take care not to twist the superior IVC. Please click here to view a larger version of this figure.
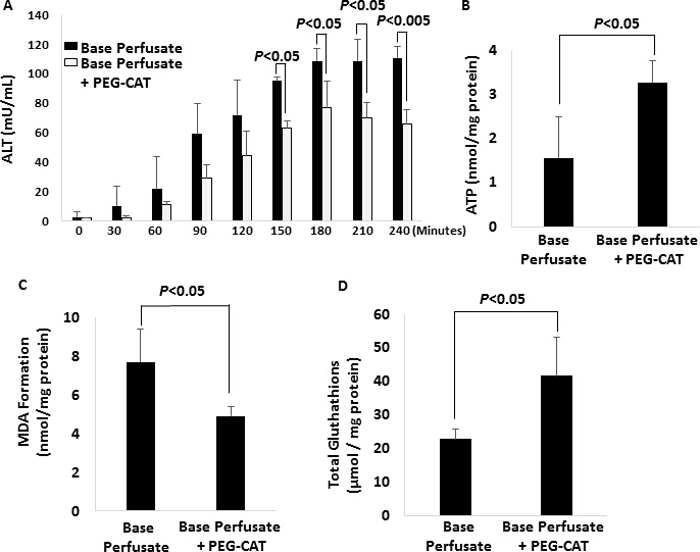
Figure 14: Analysis of tissue damage in base perfusate-only and base perfusate and plus PEG-CAT groups (N = 3/group). Error bars represent standard deviation. (A) Alanine aminotransferase (ALT) Levels. In comparing ALT levels between the base perfusate and base perfusate plus pegylated-catalase (PEG-CAT) group, there is significantly less ALT in the base perfusate plus PEG-CAT group at 150, 180, 210, and 240 min (p <0.05). (B) Adenosine Triphosphate Levels. Tissue adenosine triphosphate (ATP) was maintained in the base perfusate plus PEG-CAT group in comparison to the base perfusate alone group (p <0.05). (C) Malondialdehyde Levels. Tissue malondialdehyde (MDA) production was significantly higher in the base perfusate group than in the base perfusate plus PEG-CAT group (p <0.05). (D) Glutathione Levels. Total glutathione (GSH) was maintained in the base perfusate plus PEG-CAT group in comparison to the base perfusate alone group (p <0.05). Please click here to view a larger version of this figure.
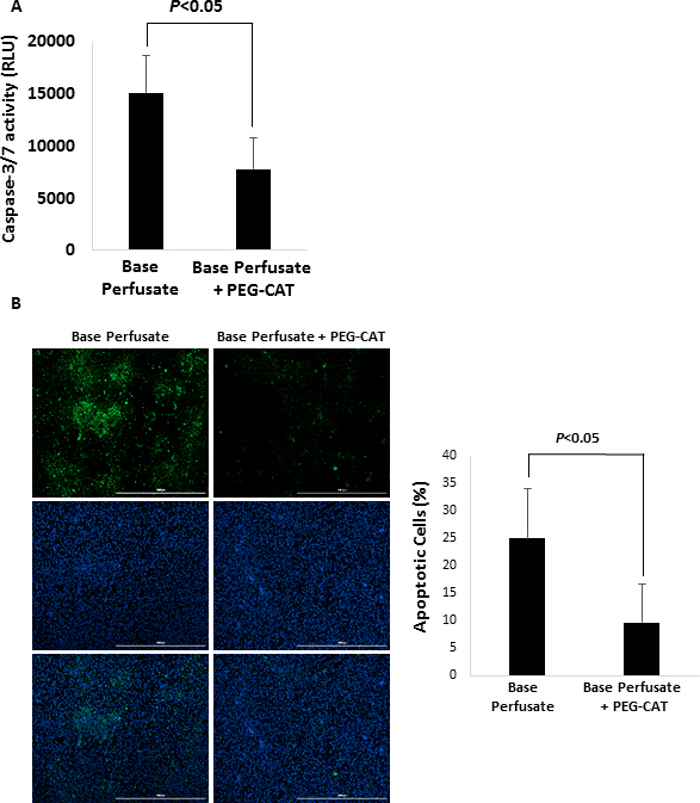
Figure 15: Analysis of apoptosis in base perfusate-only and base perfusate and plus PEG-CAT groups (N = 3/group). Error bars represent standard deviation. (A) Caspase-3/7 Activity.Caspase 3/7 activity was significantly decreased in the base perfusate plus PEG-CAT group in comparison to the base perfusate alone group (p <0.05). (B) Terminal deoxynucleotidyl transferase (TdT) dUTP Nick-End Labeling (TUNEL) staining. Images were taken using a 4X fluorescent microscope. The percentage of apoptotic cells was significantly less in the base perfusate plus PEG-CAT group in comparison to base perfusate (p <0.05). Green: apoptotic cells. Blue: nuclear. Scale bars = 1,000 µm. TUNEL positive cells were quantified by counting cells from 4 random microscopic fields. Please click here to view a larger version of this figure.
