In this manuscript, plCSA-BP-conjugated nanoparticles loaded with MTX (plCSA-MNPs) or ICG (plCSA-INPs) were intravenously injected into pregnant mice. In vivo imaging revealed strong ICG signals in the region of the uterus 30 min after plCSA-INP injection. The INPs were mainly localized to the liver and spleen region (Figure 1A). At 48 h after plCSA-INP injection, pregnant mice were sacrificed, revealing ICG signals only in the placenta, while with no signals were detectable in the fetus (Figure 1B).
We then used HFUS to monitor embryo development after the intravenous injection of nanoparticles. Biometric measurements included the gestational sac length (GS), fetal crown rump length (CRL), biparietal diameter (BPD), abdominal circumference (AC), placental diameter (PD), placental thickness (PT), umbilical artery peak velocity (UA), and fetal heart rate (HR) (Movie 1). The morphological parameters measured at different gestational ages are listed in Table 2. In the plCSA-MNP group, relative to the PBS group, the mean fetal abdominal circumference and umbilical artery peak velocity were significantly decreased at E12.5 (Figures 2A and 2H), and the crown rump length and placental diameter were significantly decreased at E10.5 (Figures 2B and 2F). Beginning on E9.5, the gestational sac length was also significantly decreased (Figure 2C), and the biparietal diameter, placental thickness, and fetal heart rate began to dramatically decrease on E 11.5 relative to those in the PBS group (Figures 2D, 2E and 2G). These findings together suggest that plCSA-MNPs have a strong cytotoxic effect on both fetal and placental development. Interestingly, treatment with MNPs also slightly impaired fetal and placental development (Figures 2A-2H), indicating that nanoparticles might improve the delivery of MTX to the placenta via the enhanced permeability and retention (EPR) effect.
| Gestational age | Group | Decidua (mm) | GS (mm) | CRL (mm) | BPD (mm) | AC (mm) | PD (mm) | PT (mm) | HR (bpm) | UA (mm/s) |
| E6.5 | 0.92±0.23 | / | / | / | / | / | / | / | / | |
| E7.5 | PBS | / | 0.82±0.24 | 0.72±0.18 | / | / | / | / | / | / |
| MNPs | / | 0.83±0.14 | 0.83±0.14 | / | / | / | / | / | / | |
| plCSA-MNPs | / | 0.65±0.23 | 0.65±0.23 | / | / | / | / | / | / | |
| E8.5 | PBS | / | 2.02±0.54 | 1.88±0.40 | 0.93±0.23 | / | / | / | / | / |
| MNPs | / | 1.49±0.50 | 1.49±0.50 | 0.82±0.20 | / | / | / | / | / | |
| plCSA-MNPs | / | 1.14±0.46 | 1.02±0.42 | 0.83±0.18 | / | / | / | / | / | |
| E9.5 | PBS | / | 3.31±0.62 | 3.49±0.65 | 1.39±0.54 | / | / | / | / | / |
| MNPs | / | 2.34±0.68 | 2.23±0.49 | 0.98±0.34 | / | / | / | / | / | |
| plCSA-MNPs | / | 1.83±0.42 | 1.59±0.59 | 0.94±0.25 | / | / | / | / | / | |
| E10.5 | PBS | / | 4.43±0.67 | 4.97±0.80 | 2.10±0.61 | 4.83±1.40 | 2.91±0.23 | 2.24±0.24 | 100±30 | 30.16±9.40 |
| MNPs | / | 3.28±0.64 | 2.91±0.83 | 1.46±0.54 | 3.95±1.28 | 2.66±0.33 | 2.17±0.19 | 87±21 | 24.63±7.35 | |
| plCSA-MNPs | / | 2.64±0.66 | 2.17±0.85 | 1.12±0.33 | 3.82±1.13 | 2.13±0.35 | 1.94±0.15 | 83±22 | 15.37±5.70 | |
| E11.5 | PBS | / | 5.68±0.73 | 6.45±0.90 | 3.08±0.70 | 8.67±2.08 | 4.16±0.39 | 2.75±0.26 | 124±28 | 31.62±7.76 |
| MNPs | / | 4.36±0.39 | 3.74±1.2 | 2.31±0.53 | 6.69±1.85 | 3.56±0.40 | 2.39±0.23 | 106±22 | 25.20±6.18 | |
| plCSA-MNPs | / | 3.42±0.76 | 2.61±0.84 | 1.51±0.54 | 4.59±1.57 | 2.54±0.49 | 2.09±0.27 | 79±20 | 16.66±5.69 | |
| E12.5 | PBS | / | / | 8.12±1.29 | 3.90±0.65 | 12.43±2.48 | 5.37±0.42 | 3.14±0.24 | 141±26 | 40.62±10.89 |
| MNPs | / | / | 4.87±1.29 | 2.87±0.62 | 8.29±1.78 | 4.25±0.67 | 2.65±0.26 | 119±18 | 27.76±7.52 | |
| plCSA-MNPs | / | / | 3.2±1.28 | 1.75±0.60 | 5.47±1.39 | 3.05±0.50 | 2.28±0.26 | 72±22 | 18.76±7.20 | |
| E13.5 | PBS | / | / | 10.04±1.2 | 4.67±0.65 | 15.64±2.33 | 6.03±0.60 | 3.49±0.23 | 157±28 | 54.62±12.37 |
| MNPs | / | / | 6.17±1.29 | 3.37±0.55 | 9.39±1.88 | 4.77±0.69 | 2.92±0.43 | 109±22 | 35.84±9.49 | |
| plCSA-MNPs | / | / | 3.57±1.71 | 1.87±0.73 | 6.25±1.41 | 3.42±0.63 | 2.37±0.34 | 60±23 | 20.02±11.20 | |
| E14.5 | PBS | / | / | 12.35±1.6 | 5.36±0.71 | 18.38±2.53 | 6.70±0.64 | 3.75±0.35 | 167±27 | 71.48±10.72 |
| MNPs | / | / | 7.6±1.56 | 3.90±0.70 | 10.31±2.31 | 5.23±0.76 | 3.10±0.39 | 99±23 | 45.80±13.07 | |
| plCSA-MNPs | / | / | / | / | / | / | / | / | / |
Table 2. Measure morphologic parameters of each gestational age. GS: Gestational sac length; CRL: Crown rump length; BPD: Biparietal diameter; AC: Abdominal circumference ; PD: Placental diameter; PT: Placental thickness; HR: Fetal heart rate; UA: Umbilical artery peak velocity; /: cannot measure.
We next measured MTX concentrations in the placentas and fetuses using HPLC. Using the HPLC operation parameters described above, the MTX retention time was determined to be 7 min, and MTX was detected in the placentas of the plCSA-MNP group (Figure 3). The MTX concentrations in placentas and fetuses were determined using MTX standard curves (Figure 4). 24 h after injection, the placental MTX level in the MNP group was significantly lower than that in the plCSA-MNP group, and no MTX was detected in fetuses of the plCSA-MNP group. MTX could still be detected in the placenta 48 h after plCSA-MNP injection (Figure 5). These results demonstrate that plCSA-MNPs cannot cross the placenta, thus minimizing potential adverse effects on the fetus.
In summary, this three-method system comprised of in vivo fluorescence imaging, HFUS, and HPLC can be employed to determine how well a drug delivery vehicle targets nanocarriers and delivers drugs to the placenta. Using these methods, we have demonstrated that plCSA-BP guided nanoparticles are an efficient tool for targeting the delivery of drugs to the placenta.
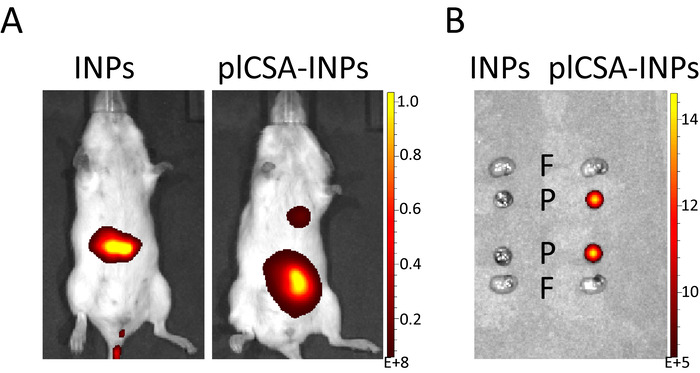
Figure 1. In vivo fluorescence imaging. (A) Pregnant mice (n=5 each) at E11.5 were injected with INPs or plCSA-INPs (ICG equivalent 5 mg/kg) via the tail vein. After 30 min, the mice were imaged using a fluorescence imaging system. (B) 48 h after the injection of INPs or plCSA-INPs, the fetuses (F, n=2 per mouse) and placentas (P, n=2 per mouse) were collected and imaged with a fluorescence imaging system. Please click here to view a larger version of this figure.
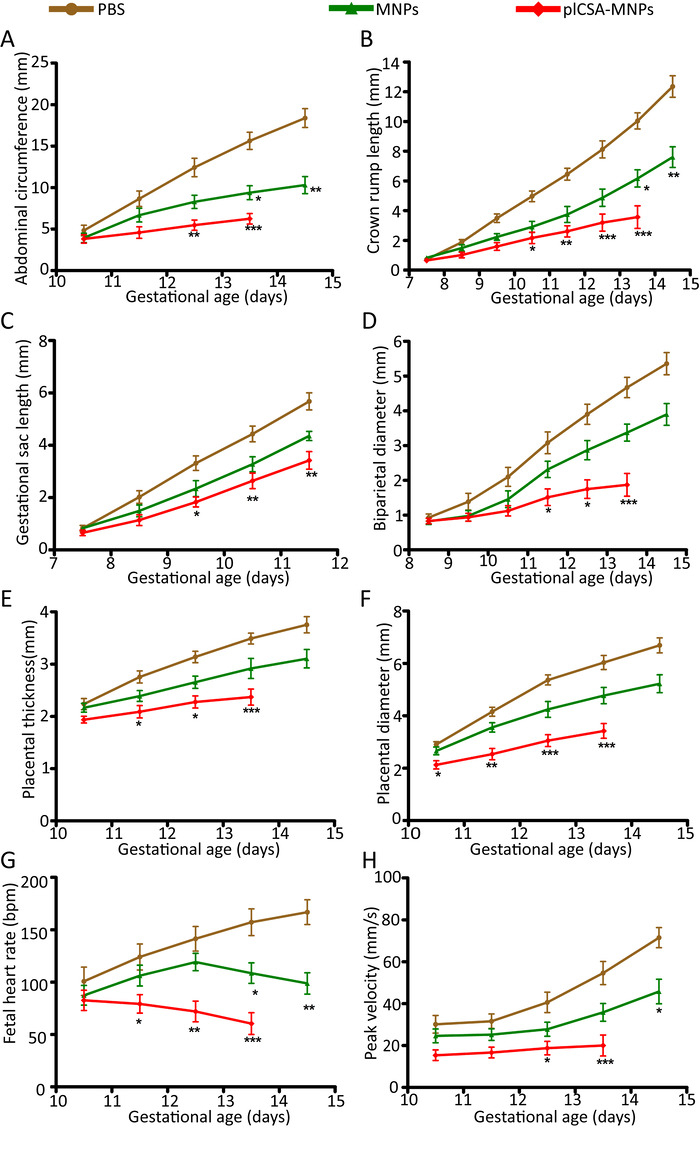
Figure 2. Quantification of embryonic growth by HFUS. (A) The abdominal circumference (n = 30-51 embryos/day), (B) crown rump length (n = 30-51 embryos/day), (C) gestational sac length (n = 10-30 embryos/day), (D) biparietal diameter (n = 30-51 embryos/day), (E) placental thickness (n = 30-51 embryos/day), (F) placental diameter (n = 30-51 embryos/day), (G) fetal heart rate (n = 20-33 embryos/day), and (H) umbilical artery peak velocity (n = 12-36 embryos/day) as measured non-invasively by ultrasound in vivo. All tests were compared by 2-tailed paired t-test, and p < 0.05 was considered statistically significant. Values are expressed as the means ± SD. *p < 0.05, **p < 0.01, ***p < 0.001 compared to the PBS group. Please click here to view a larger version of this figure.
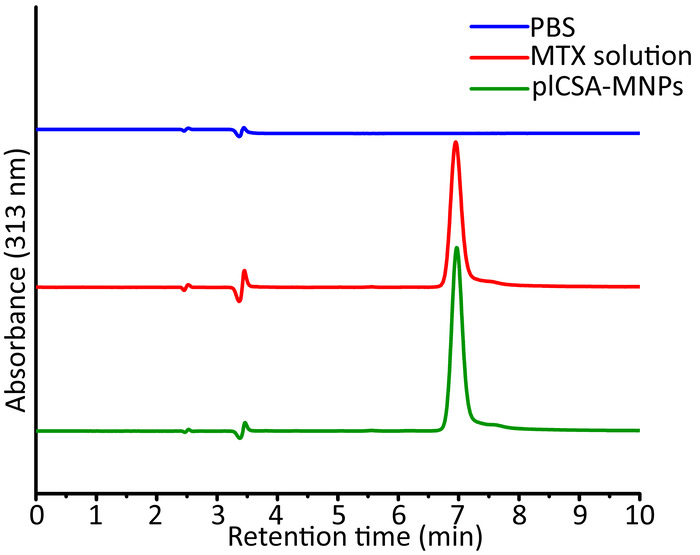
Figure 3. Representative HPLC chromatograms of placental samples. Pregnant mice (n=5 each) were intravenously injected with PBS or plCSA-MNPs, and their placentas (n=15 each group) were collected 24 h later for HPLC. Using a standard solution of MTX with UV detection at 313 nm, the retention time was determined to be 7 min. Please click here to view a larger version of this figure.
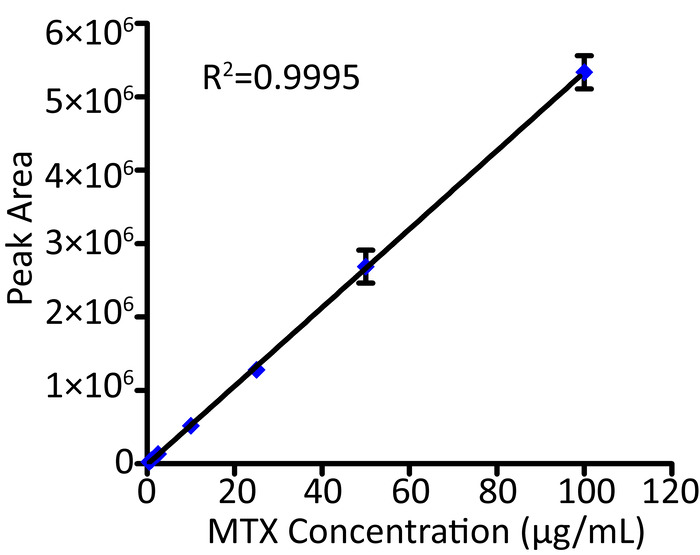
Figure 4. Standard curves for MTX. The concentrations of MTX ranged from 0.5 μg/mL to 100 μg/mL. The data represent the mean ±SD for n=3. The error bars of some data are smaller than the rhombic symbols. Please click here to view a larger version of this figure.
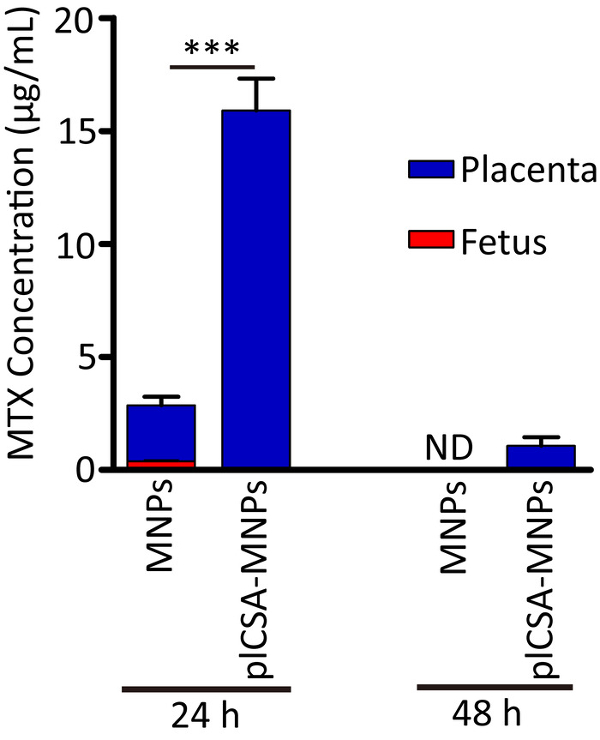
Figure 5. Application of HPLC to determine the biodistributions of nanoparticles in placentas and fetuses. Pregnant mice were administered a single injection of MNPs or plCSA-MNPs (1 mg/kg MTX equivalent) at gestational stage E13.5. After 24 h and 48 h, the concentrations of MTX in the placentas (n = 15) and fetuses (n = 15) were measured by HPLC. Values are expressed as the means±SD. Differences in MTX concentrations between the MNP and plCSA-MNP groups were analyzed using unpaired Student's t-test (***p < 0.001); nd: not detected. Please click here to view a larger version of this figure.
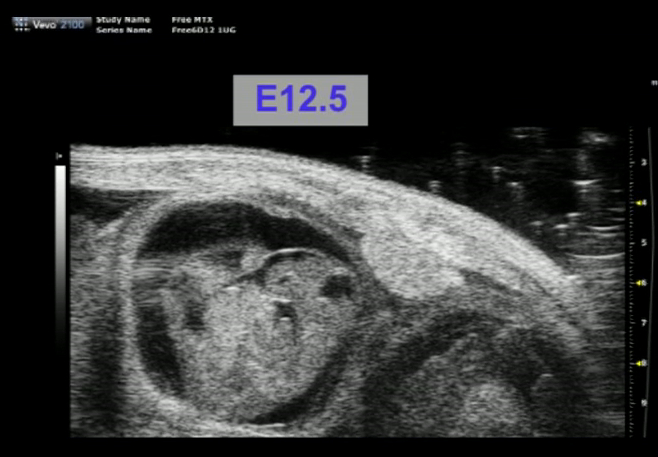
Movie 1. HFUS images of fetuses and placentas illustrating biometric measurement locations. Please click here to view this video. (Right-click to download.)
