The experiments were performed on male Wistar Kyoto rats according to Directive 2010/63 EU on the protection of animals used for scientific purposes and were approved by the I Local Bioethical Committee in Warsaw.
1. Insertion of the Line for Intraintestinal Administration
NOTE: Here we propose intracolonic administration of a marker using a catheter. It may be modified by oral administration or gavage at various levels of the digestive tract e.g. stomach or duodenum. Remember to use disposable surgical clothing, including surgical gown, hood and gloves, and ensure to follow the safety precautions related to the sharp tools used in surgery (needles, etc.) during procedures 1-6.
- Fast animals overnight before the procedure. Perform all procedures during general anesthesia, i.e., obtained by injection of urethane 1.5 g/kg bw i.p. Assess proper anesthetization by the lack of palpebral and corneal reflexes, and by toe-pinch and tail-pinch method.
- Use a pediatric Foley catheter (10F or 8F) as a colonic catheter. Mark the catheter to indicate the part that will be inserted into the colon (approximately 8 cm).
- Check the anal region and the stool content in the rectum before inserting the catheter into the colon. If stool is present, empty the rectum by massaging the rectal area.
- Put a lubricant (e.g. glycerin or petrolatum) along the catheter. Moisten the anus and its surroundings with the lubricant.
- Insert the catheter with a guide wire approximately 8 cm through the external anal sphincter. Make slow forward-backward and circular movements.
NOTE: Keep on checking the location of the catheter by abdominal palpation while inserting the catheter.
2. Inferior Vena Cava Catheterization
- Shave fur in the groin. Alternately disinfect the skin with alcohol and povidone iodine 3 times and cover the groin area with surgical drapes.
- Try to feel the pulse on the femoral artery and cut the skin longitudinally for the length of about 2.0 cm in the place where the pulse is palpable.
- Dissect the fascia and muscles to visualize the neurovascular bundle.
- Dissect the femoral vein from the neurovascular bundle: first nerves, then the femoral artery, and then the vein.
NOTE: Be careful during the dissection of the neurovascular bundle, since tiny branches of the femoral vein may easily be damaged, producing bleeding. - Put two ligatures on the femoral vein. Do not tie the knots yet. Catch the ends of the proximal ligature with a needle holder.
- Carefully pull the ligature ends with the holder upwards to close the proximal part of the vein. Wait until the vein is filled with blood and tie the distal knot.
- Make a small incision (ca. 1 mm) on the vein between the knot and proximal ligature, using microsurgical scissors. Insert the catheter using tweezers or the needle with the curved end.
NOTE: Puncture the vein and use the bended tip of the needle as a guide for the catheter. Loosen the proximal ligature while inserting the catheter. Insert the catheter for 6-7.0 cm. - Secure the catheter in the femoral vein with two single surgical knots. Tie the proximal ligature as well.
- Check the patency of the catheter by attempting to draw blood with a syringe. Rinse the catheter with 0.3 mL of the heparinized saline (100 units/mL).
- Close the surgical wound with two layers of single stitches.
3. Portal Vein Catheterization
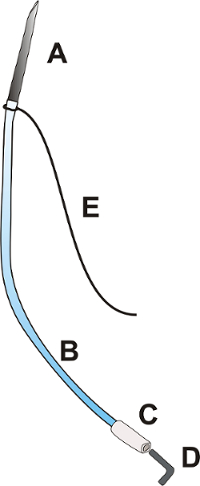
Figure 1: Portal catheter. The portal catheter consists of a needle OD: 0.9 mm with a length of about 25.0 mm [A], a flexible polyurethane catheter OD: 0.025", length about 100.0 mm [B], a flexible polyethylene tip of the catheter OD: 0.040", approximately 15.0 mm long [C], a plug [D], and a ligature 3/0 with a length of 100.0 mm [E]. Please click here to view a larger version of this figure.
- Prepare the portal catheter according to Figure 1.
- Insert the cut end of the needle (OD: 9 mm) into the polyurethane catheter OD: 0.025".
- Tie the ligature 3/0 at the junction of the needle and catheter.
NOTE: Ensure that the longer part of the ligature is at least 6 cm long. - Insert the end of the catheter OD: 0.025" into the polyethylene catheter OD: 0.040".
- Close the catheter with a metal or plastic plug.
- Midline laparotomy
- Shave fur in the abdomen, alternately disinfect the skin with alcohol and povidone iodine 3 times, and cover the area with surgical drapes.
- Cut the skin longitudinally from the xiphoid of the sternum to the navel.
- Cut the muscles of the abdominal wall along the white line.
- Expand the cut rostrally in the Y shape so that the xiphoid cartilage is between two cuts.
- Portal vein dissection
- Moisten the surgical swabs with saline.
- Exteriorize the cecum, ascending and transverse colon, and small intestine loop. Put the intestines on the left side to expose the root of the mesentery.
NOTE: Cover the intestines with gauze moistened with a physiological saline to protect the intestines from drying. - To expose the portal vein, carefully move the hepatic lobes to the sides or upwards towards the diaphragm with the moistened swabs.
- Localize the part of the portal vein that is not covered with the mesentery (in the hepatic hilum, about 5 mm long) and pass the ligature 3/0 (15 cm long) under the portal vein.
NOTE: To protect tissues from damage while placing the ligature, moisten the ligature with a physiological saline solution. - Clamp the ends of ligature with forceps and tighten it gently to stabilize the vessel.
- Insertion and stabilization of the catheter
- Pass the longer part of the portal catheter's ligature under the free part of the portal vein and pull it so that the catheter is located just next to the portal vein.
- Insert the needle into the upper mesenteric vein 3 mm below the junction of upper mesenteric vein and the portal vein. Hold the needle at a 30° angle and, after entering into the vein, reduce the angle and advance the needle almost horizontally, in parallel to the portal vein.
NOTE: Insert the needle for a length of approximately 6-7 mm. The stabilizing ligature should gently tighten the portal vein while inserting the catheter. - Apply 1-2 drops of tissue glue at the place where the needle is inserted. Remove the swabs that cover the liver.
- Put the intestines back into the abdominal cavity.
- Moisten the intestines with a warmed up saline solution and cover it with moistened sterile gauze.
- Check the patency of the catheter and rinse the catheter with 0.3 mL of the heparinized saline (100 units/mL).
NOTE: Venous blood spontaneously backflows in the catheter.
- Ending of the surgery
- After 5 minutes, check the color of the intestines and peristaltic movements, make sure that the proper mesenteric blood flow is maintained.
- Close the abdominal cavity with 3 stitches: wall peritoneum with the inner layer of the abdominal wall muscles – a continuous, absorbable suture; remaining muscles of the abdominal wall – a continuous, absorbable suture; skin and subcutaneous tissue – single, non-absorbable sutures.
NOTE: Exteriorize the distal part of the catheter around the navel.
4. Portal Vein Blood Sampling
- Sample portal vein blood at times according to the specific testing protocol used; see Table 1.
| Short protocol | Long protocol |
| t0 – baseline (before intracolonic administration) | t0 – baseline (before intracolonic administration) |
| t1 – 5 min after intracolonic administration | t1 – 30 min after intracolonic administration |
| t2 – 30 min after intracolonic administration | t2 – 60 min after intracolonic administration |
Table 1: Portal blood sampling protocols for gut permeability assessment.
NOTE: The time between consecutive blood sampling depends mainly on the bioavailability of the tested substances and the site of administration (colon, stomach, etc.).
- Open the portal catheter plug and let the blood flow freely.
- Use syringe (vol. 2 mL) and blunt needle OD: 0.9 mm. Collect no more than 0.7 mL of blood.
- Rinse the catheter with 0.3 mL of heparinized saline (100 units/mL) and close the catheter plug.
5. Inferior Vena Cava Blood Sampling
- Sample inferior vena cava blood at times according to the specific testing protocol used; see Table 2.
| Portal vein | Inferior vena cava |
| t0 – baseline (before intracolonic administration) | t0 – baseline (before intracolonic administration) |
| t1 – 30 min after intracolonic administration | t1 – 30 min after intracolonic administration |
Table 2: Protocol of blood sampling for liver clearance measurement and tracking the gut-portal blood-liver-systemic blood pathway.
- Open the inferior vena cava catheter plug and let the blood flow freely.
- Collect no more than 0.7 mL of blood using syringe (vol. 2 mL) and broken needle OD: 0.9mm.
- Rinse the catheter with 0.2-0.3 mL of heparinized saline (100 units/mL) and close the catheter plug.
6. Administration of a Gut Permeability Marker
- Remove the guide wire and inflate the colonic catheter balloon, using adequate volume of sterile water (usually 1 mL but check actual balloon size before insertion).
NOTE: The balloon diameter should not exceed 1 cm. - Place the rat head down (inclination about 15%) to minimize the risk of the outflow of the administered solution from the colon.
- Slowly administer the tested substance (e.g. trimethylamine, 100 mg/kg bw) using a drainage port in colonic catheter.
NOTE: Do not exceed the volume of 0.75 mL of the administered solution and the feeding speed of 0.5 mL/min to prevent the outflow of the administered solution from the anus. - After 10 min deflate the catheter balloon.
- Sample blood from the inferior vena cava and the portal vein according to the specific testing protocol used; see Table 1 and Table 2.
- Euthanize animal via approved method.
7. Calculation of Liver Clearance
- Express liver clearance, understood as hepatic extraction, by the difference between portal blood concentration and inferior vena cava blood concentration or by the ratio of inferior vena cava to portal blood concentration, (1 – (inferior vena cava concentration/portal vein concentration)).
8. Evaluation of the Test Substance Concentration n Blood Samples
- Depending on the test substance and test methodology, subject the sample to appropriate laboratory procedures (centrifugation, etc.). In the proposed protocols, we evaluate TMA/TMAO and SCFA concentration using liquid chromatography coupled with triple-quadrupole mass spectrometry. Please find a detailed description of the method in Supplemental Material.
We have successfully measured the GBB permeability and liver clearance of TMA in rats. We have demonstrated that hypertensive rats have an increased colon permeability to TMA in comparison to normotensive rats (Figure 2)4. In another study we found that high salt intake does not affect the GBB permeability and liver clearance of TMA (Figure 3)14.
Measuring the concentration of SCFA in stools, portal blood, and peripheral blood, we traced the path of the molecules from the intestine to the peripheral blood. The exemplary results for those experiments are presented in Table 3.

Figure 2: Hypertension-associated changes in gut-blood barrier permeability. Intracolonic administration of TMA produced a significant increase in portal blood TMA in each group (n=12 for each group). The increase in portal blood TMA in the hypertensive (SHR) group was significantly higher than in normotensive (WKY) group. We used the long protocol consisting of blood sampling 30 min and 60 min after TMA administration (IC TMA). Values are means, + SE, *p < 0.05 vs baseline, #p < 0.05 WKY vs SHR. This figure has been modified from Jaworska et al.4 Please click here to view a larger version of this figure.
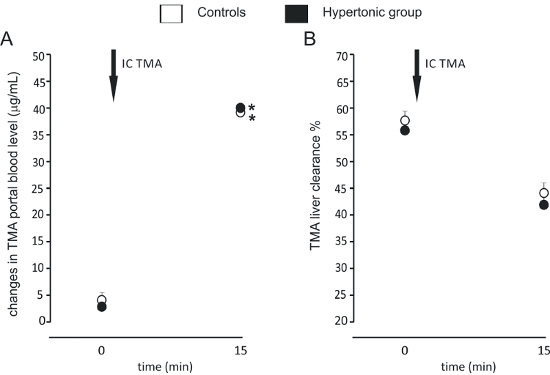
Figure 3: Gut-blood barrier permeability and liver clearance after high salt intake. (A) Intracolonic administration of TMA produced a significant increase in portal blood TMA. The size of the increase was similar between the groups (n=7 for each group). We used a simplified protocol, taking blood samples at baseline (0) and 15 min after administration of TMA (IC TMA). (B) TMA liver clearance was similar between the groups at baseline, and 15 min after the intracolonic administration of TMA. Values are means, + SE. *p < 0.05 vs baseline. This figure has been modified from Bielinska et al.14 Please click here to view a larger version of this figure.
| SCFA | Stool concentration (µM) | Portal blood concentration (µM) | Peripheral blood concentration (µM) |
| AA- acetic acid (C2) | 15998.40 ± 4317.58 | 564.22 ± 155.34 | 149.89 ± 31.74 |
| IPA- propionic acid (C3) | 5390.70 ± 1016.19 | 138.25 ± 55.50 | 5.36 ± 3.25 |
| IBA- isobutyric acid (C4) | 191.20 ± 123.87 | 4.51 ± 1.60 | 1.14 ± 1.16 |
| BA- butyric acid (C4) | 4159.80 ± 3141.68 | 143.14 ± 68.42 | 6.43 ± 4.18 |
| 2MeB- 2 methylbutyric acid (C5) | 80.90 ± 59.86 | 2.02 ± 0.88 | 1.14 ± 1.42 |
| IVA- isovaleric acid (C5) | 109.10 ± 56.05 | 2.59 ± 1.07 | 0.90 ± 1.22 |
| VA- valeric acid (C5) | 281.9 ± 158.20 | 8.55 ± 3.56 | 0.72 ± 1.02 |
| ICA- isocaproic acid/ 4-methylvaleric acid (C6) | 5.9 ± 2.95 | 0.61 ± 0.15 | 1.76 ± 0.87 |
| CA- caproic acid (C6) | 287.00 ± 309.68 | 11.19 ± 4.94 | 1.12 ± 0.93 |
Table 3: SCFA concentration in stool, portal blood, and peripheral blood (n=7).
| Test substance | Possible application |
| Bacterial metabolites: trimethylamine (TMA), short chain fatty acids (SCFA), hydrogen sulfide, etc. |
GBB permeability studies Tracking a gut-portal blood-liver-systemic blood pathway Hepatic clearance studies |
| Classic permeability markers: FITC-dextran, polysaccharides, PEG, etc. |
GBB permeability studies |
| Drugs | absorption and hepatic clearance studies |
Table 4: Exemplary test substances with possible applications.
