The protocol described allows the characterization of surface markers of innate and adaptive immune cells isolated from murine perigonadal adipose tissue and liver in a model of diet-induced NASH. In this model, NASH was induced by administration of HFD plus sucrose (6%) in drinking water for 7 to 15 weeks in C57Bl/6J mice, as previously reported13. Importantly, mice were housed in semi sterile conditions and, thus, exposed to environmental antigens throughout the experiment. HFD fed mice housed in SPF conditions and chow diet mice housed under SPF and non-SPF conditions served as controls. HFD feeding resulted in significant body weight gain already after 7 weeks in both groups. A significant difference in body weight was first evident at week 4 (P < 0.001) and remained significant throughout the following experimental weeks. However, no significant differences in weight gain were shown between SPF and non-SPF mice after 7 weeks13. The stromal vascular fraction and immune cells from perigonadal adipose tissue and livers of male mice fed a HFD for 7 weeks were isolated by collagenase digestion. Immune cells were labeled with fluorophore-conjugated primary antibodies and proportions of T cells, B cells, macrophages, NK cells, dendritic cells and granulocytes were quantified via flow cytometry analysis. Gating for T cell subpopulations, including doublet discrimination, and viability staining, in murine perigonadal fat is illustrated in Figure 1. CD45+ leucocytes are first gated for CD4 and CD8 and subsequently gated for CD44 and CD62L to discriminate between naïve, central memory, effector memory and effector T cells. CD44+ cells were then further characterized with CD127, KLRG1 and PD-1. Figure 2 provides the gating strategy for analyzing B cells, granulocytes, NK cells, macrophages and dendritic cells.
Representative results of extracellular staining of T cells within murine liver of HFD exposed mice compared to HFD SPF mice are demonstrated in Figure 3A. Indeed, a higher percentage of effector memory CD4+ and CD8+ T cells can be detected in HFD exposed mice, whereas intrahepatic naïve CD4+ and CD8+ T cells were found to be considerably lower in exposed compared to SPF mice at week 7 (Figure 3A).
To validate these results, the hepatic inflammatory response associated with antigen exposure was investigated by hematoxylin/eosin staining of liver sections of 15 weeks fed mice13. Severe steatosis, including increase of large lipid droplets resulting in macrovesicular steatosis, lobular inflammation, hepatocellular ballooning and destroyed lobular structure, was found in HFD exposed mice while only some SPF mice displayed a mild fat accumulation in the liver (Figure 3B). As reported in Figure 3C, the percentage of NK cells was higher in perigonadal adipose tissue of HFD exposed mice, whereas HFD SPF mice showed higher percentages of dendritic cells. No significant differences were found for macrophages and monocytes. Altogether, these results confirm more severe hepatic steatosis in HFD exposed mice and minor differences in adipose tissue between HFD exposed and SPF mice.
Table 1 shows the antibodies used in panel 1. Antibodies used in flow cytometry analysis for extracecullar staining of B cells, macrophages, NK cells, dendritic cells and granulocytes are depicted in Table 2.
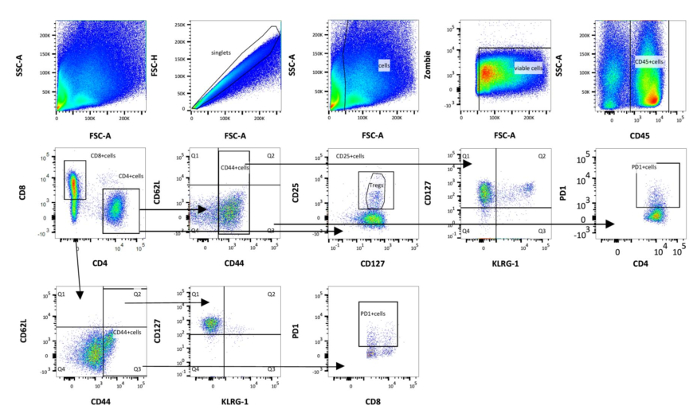
Figure 1: Schematic representation of gating strategy used in flow cytometry analysis of adipose immune cells (panel 1). First, the cells are gated on singlets. Then, debris is excluded by using forward scatter area (FSC-A) and side scatter area (SSC-A) and choosing the correct size. Cells are further characterized by the expression of CD45. Viable cells are selected using alive/dead cell marker that is an amine reactive fluorescent dye that is non-permeant to live cells, but permeant to the cells with compromised membranes. T cells were divided into cytotoxic T cells (CD8+) and T-helper cells (CD4+) and subdivided into naïve (CD44+CD62L–), central memory (CD44+CD62L+), effector memory (CD44+CD62L–) and effector (CD44–CD62L+) T cells. Finally, CD44+ cells are gated on KLRG1, CD127 and PD-1. Please click here to view a larger version of this figure.
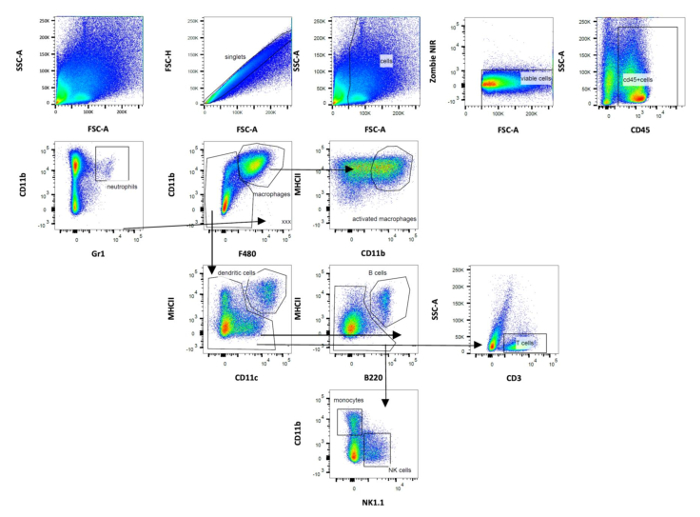
Figure 2: Schematic representation of gating strategy used in flow cytometry analysis of adipose immune cells (panel 2). Gating of dendritic cells was based on CD11b and CD11c expression. The following other populations were defined: B cells, NK cells, macrophages, monocytes and granulocytes. Data were analyzed after acquisition with the appropriate software. Please click here to view a larger version of this figure.
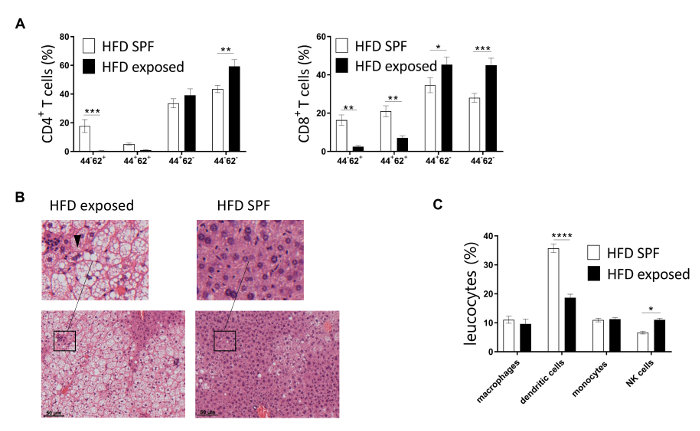
Figure 3: Representative flow cytometry analysis of T cells isolated from murine perigonadal adipose tissue and liver. (A) CD4+ and CD8+ T cells of murine livers from 7 week HFD mice maintained under SPF and exposed conditions were analyzed via flow cytometry. (B) Representative staining of 15 week HFD SPF and exposed mice. Infiltration of immune cells and ballooned hepatocytes (arrowhead) illustrate NASH. (C) Percentages of adipose innate immune cells as percentage of leukocytes in HFD mice maintained under SPF or exposed conditions for 7 weeks. n = 6-10 mice per group. Significance was determined using two-way ANOVA multiple measurement. Data are represented as mean ± SEM. ** P <0.01, *** P < 0.001. This figure has been modified from refefence13. Please click here to view a larger version of this figure.
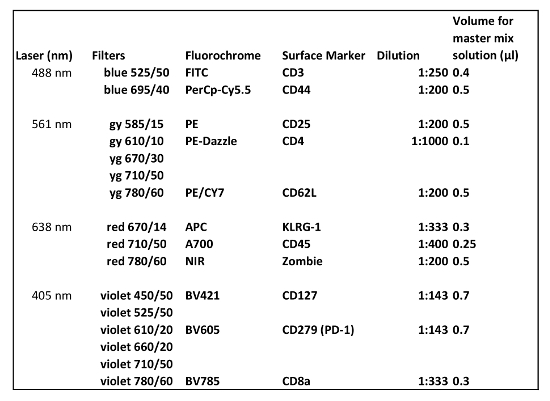
Table 1: Antibodies used in flow cytometry for extracellular staining (Panel 1). The amount of antibody described is for the analysis of one sample.
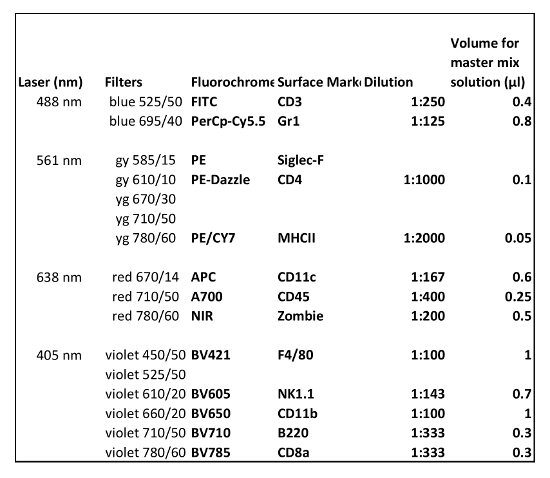
Table 2: Antibodies used in flow cytometry for extracellular staining (Panel 2). The amount of antibody described is for the analysis of one sample.
