The protocol (No. 31771319) was approved by the Hebei Normal University Review Board and conformed to the Declaration of Helsinki. All participants provided written informed consent before participating in the testing described.
1. Participant Screening and Preparation for the Experiment
- For recruitment, ensure that the participants satisfy the following inclusion criteria: aged between 18 and 25, a minimum body mass index (BMI) of 23 kg/m, which is the overweight cut-off for Asian adults10, consistent body weight (± 2 kg) for the most recent three months, no exercise training or regular physical activities, no record of hormonal, orthopaedic or cardiovascular diseases, diabetes, hyperlipidaemia, hypertension or polycystic ovary syndrome, as well as, no current use of prescribed medications (including contraceptive pills) and no history of smoking.
- Randomly assign 47 eligible participants to one of the following four groups: traditional HIE (n = 12), sprint interval exercise (SIE, n = 11), repeated sprint exercise (RSE, n = 12) or MCE (n = 12) group.
- Adjust and record the appropriate seat height on the cycling ergometers so that the participant pedals with a slight knee bend (~10°) at full downstroke of the pedal.
- Instruct the participants to perform two initial exercise sessions (as described in step 3) to familiarize them with the respective type of cycling exercise (HIE, SIE, RSE or MCE).
2. Experimental Procedures
- First, instruct each participant to perform a continuous incremental test on a stress testing cycle ergometer to assess maximal oxygen uptake (V̇O2max).
- Warm up for 5 min at 25 W. Then start the test by performing continuous 2 min stages (20 W increment per stage) starting at 50 W with a pedal frequency of 60 rpm until volitional exhaustion.
- Use a breath-by-breath metabolic analyzer to measure the oxygen consumption during the exercise.
- Calculate the V̇O2max based on the highest 30 s average value. Then, calculate a power output that elicits 60%, 90% and 120% V̇O2max in the MCE, HIE and SIE groups, respectively, using the equation of linear regression through plotting the steady state V̇O2 versus power output11.
- At least 5 days after pre-intervention assessments, instruct the HIE, SIE, RSE and MCE groups to commence their respective training.
NOTE: Start all exercise tests at the same time of the day (e.g., 11:00 A.M.). Meanwhile, ensure that the tests are conducted in a laboratory with temperature and humidity-controlled settings (20 °C and 50% relative humidity). Ask all participants to stick to both their daily activities and eating habits throughout the experiment.- Instruct the participant to refrain from any strenuous exercise for 48 h, after a routine warm-up, instruct the HIE, SIE, RSE and MCE groups to engage in their respective exercise session on a cycle ergometer as arranged. Perform the exercise protocol as detailed in step 3.
- Perform 6 exercise sessions carried out over a time span of 10 days for all four groups. Select the 1st (1ST) and 6th (6TH) exercise sessions to observe the cTnT response to the acute exercise (Figure 1).
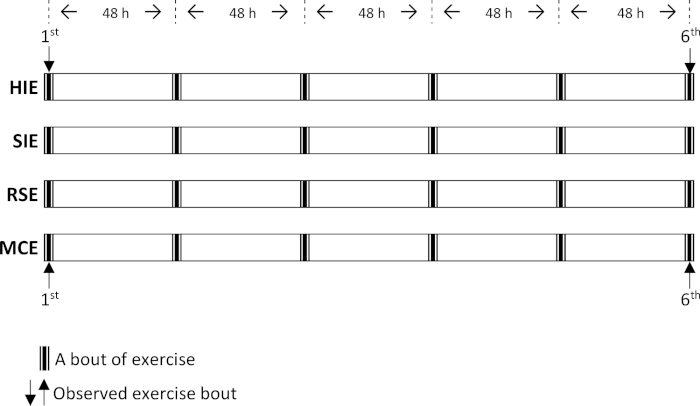
Figure 1: Schematic diagram of study procedures. HIE = high-intensity interval exercise; SIE = sprint interval exercise; RSE = repeated sprint exercise; MCE = moderate-intensity continuous exercise. Please click here to view a larger version of this figure.
- Record a continuous electrocardiogram (ECG) during exercise via a portable electrocardiograph (ECG) monitor.
- Draw venous blood samples before and immediately after exercise, as well as 3 h and 4 h after the selected exercise session to assess the serum cTnT. With the subjects in a seated position, draw 5 mL of venous blood from the antecubital vein for each sample.
NOTE: Post-exercise blood samples timings conformed to our prior work, which demonstrated that blood cTnT concentrations reached their peak 3 or 4 h following acute exercise in a laboratory-based study12. - For the separation of the serum, allow the blood to clot at room temperature. Centrifuge the blood samples at 3,500 x g for 20 min.
- Aspirate the serum and store at -80 °C for the subsequent analysis of cTnT.
- Use an analyzer to perform the quantitative measurement of the cTnT with a high sensitivity immunoassay based on electrochemiluminescence technology. Take 1 mL of the serum and put it into a special test tube for measuring cTnT. Then insert the tube in the analyzer and press the start button.
NOTE: The human cTnT protein itself consists of 288 amino acids. Two monoclonal antibodies are used for the assay which are specifically directed against human cardiac troponin T. The antibodies recognize the central part of cardiac troponin T protein4, specifically targeting two epitopes at amino acid positions 125-131 and 136-147.
3. Exercise Protocols
- In each exercise session, instruct the 4 groups to follow the steps below.
- Complete an identical 10 min warm-up at 50-60% of HRmax (percentage of individual maximal heart rate during exercise session) and 5 min cool down at 20 W.
- Following the warm-up. Have a 2 min recovery period, where participants remain seated but stationary on the cycle ergometer.
- Direct the participants to accelerate as soon as possible at the beginning of each exercise bout to reach the intended intensity. During this time a researcher sets the respective exercise protocol in a PC computer and then counts down, "5-4-3-2-1-Go!". At the command of "Go!", participants start to exercise and activate the computerized system.
NOTE: For the MCE, HIE and SIE, accelerate to the planned intensity (see step 2.1.3), i.e. 60%, 90% and 120% V̇O2max, respectively. For the RSE, accelerate to “all-out” exercise (see step 3.4). The ergometer is linked to a PC computer with specific software. - Instruct the participants to remain seated while cycling and secure their feet to the pedals using toe clips, and verbally encourage the participants to give a maximal effort to exercise at the desired intensity throughout each session.
- HIE protocol: Repeat 4 min bouts of exercise on a stress testing cycle ergometer at an intensity of 90% V̇O2max, followed by a 3 min passive recovery (complete rest) until the targeted 200 kJ of work is achieved.
- SIE protocol: Repeat 1 min bouts of exercise on a stress testing cycle ergometer at an intensity of 120% of V̇O2max, followed by a 1.5 min passive recovery until the targeted 200 kJ of work is achieved.
- RSE protocol: Repeat 6 s “all-out” sprints interspersed with 9 s passive recovery periods on a Wingate testing cycle ergometer, with a resistance of 1.0 kg until the targeted 40 repetitions are achieved, and the total mechanical work was recorded.
- MCE protocol: Perform continuous cycling exercise, until a target of 200 kJ of work is achieved, at an intensity of 60% V̇O2max.
4. Statistical Analyses
- Perform data analysis using a statistical software package. Evaluate the normality of the data using the Kolmogorov–Smirnov test12. Use P < 0.05 for assessing statistical significance.
- Compare the differences in HRmean (mean heart rate during exercise session) and %HRmax across the four groups (HIE, SIE, RSE and MCE) and the two observed exercise sessions (1ST and 6TH) using two-way ANOVA, with repeated measures. Use the Newman–Keuls post-hoc test for cases in which the main effect is significant.
- Compare cTnT across the time points (pre-exercise and peak post-exercise) and two observed exercise sessions (1ST and 6TH) using the non-parametric Wilcoxon signed ranks test because of the skewed distribution of the cTnT data. Further, the Kruskal-Wallis test was used to assess the statistical significance of differences in cTnT levels across the four groups (HIE, SIE, RSE and MCE), and the Mann-Whitney U test was used for pairwise comparisons where appropriate.
All participants (n = 47) completed the study, and no adverse cardiac events (e.g., chest pain and sign of myocardial ischemia on ECG) were found during testing in the four groups. As expected, the acute exercise heart rate (HR) data, including HRmean and %HRmax, at the 1ST assessment is similar (all P > 0.05) to those in the 6TH assessment in all four groups. Further, the HR data in the RSE and MCE groups is the highest and lowest among the four groups, respectively, but is similar between the HIE and SIE groups (Table 1).
| Powerexe | Timeexe | Workexe | HRmean | %HRmax | |
| (W) | (min) | (KJ) | (beat.min-1) | ||
| HIE (n=12) | |||||
| 1ST | 119 ± 12 | 28 ± 3 | 200 ± 0 | 157 ± 9 | 85 ± 4 |
| 6TH | 119 ± 12 | 28 ± 3 | 200 ± 0 | 155 ± 6 | 84 ± 4 |
| SIE (n=11) | |||||
| 1ST | 160 ± 18 | 21 ± 2 | 200 ± 0 | 148 ± 11 | 85 ± 4 |
| 6TH | 160 ± 18 | 21 ± 2 | 200 ± 0 | 147 ± 7 | 85 ± 5 |
| RSE (n=12) | |||||
| 1ST | 193 ± 17‡ | 4 ± 0‡ | 46 ± 4‡ | 169 ± 5‡ | 94 ± 7‡ |
| 6TH | 204 ± 15*‡ | 4 ± 0‡ | 49 ± 4*‡ | 171 ± 8‡ | 95 ± 6‡ |
| MCE (n=12) | |||||
| 1ST | 54 ± 10† | 63 ± 12† | 200 ± 0 | 140 ± 12† | 76 ± 6† |
| 6TH | 54 ± 10† | 63 ± 12† | 200 ± 0 | 137 ± 11† | 74 ± 6† |
Table 1: Acute exercise data. Data are presented as the mean ± SD. HIE, high-intensity interval exercise; SIE, sprint interval exercise; RSE, repeated sprint exercise; MCE, moderate-intensity continuous exercise; 1ST, the 1st exercise session; 6TH, the 6th exercise session; Powerexe, power output during exercise; Timeexe, total exercise duration; Workexe, work output during exercise; HRmean, mean heart rate during exercise session; %HRmax, percentage of individual maximal heart rate during exercise session.*Significantly different from the corresponding value of 1ST, P < 0.05; †Significantly different from the corresponding value of HIE, SIE, and RSE, P < 0.05; ‡Significantly different from the corresponding value of HIE and SIE, P < 0.05; This table has been modified from Nie et al.13 and Zhang et al.14.
Figure 2 reveals the acute exercise cTnT data on all four groups across the 10-day period, which are shown in the form of individual data points for pre-exercise (Pre-exe) and peak post-exercise (Post-exe) values. The cTnT concentration is discovered to be on the rise following acute exercise (P < 0.05) at the 1ST and 6TH assessments in all four groups. Moreover, no differences in cTnT concentration are found among the groups except for the smaller response after RSE at the 1ST. Moreover, the cTnT concentration at the 6TH assessment before MCE is higher than that at the 1ST assessment before MCE and at the 6TH assessment before RSE (both P < 0.05).
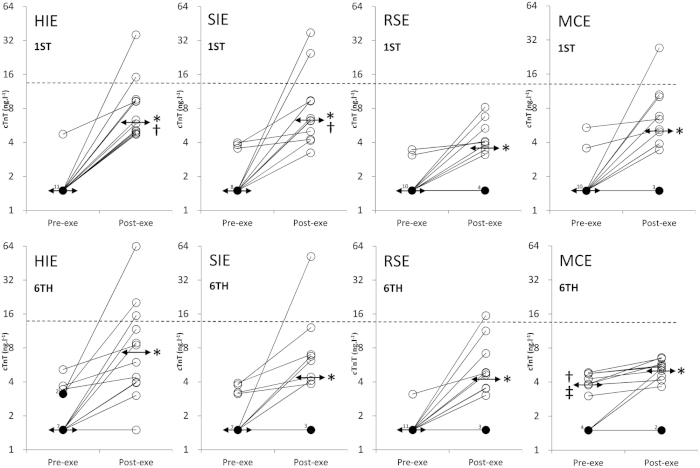
Figure 2: Pre-exercise (Pre-exe) and peak post-exercise (Post-exe) cardiac troponin T concentrations (cTnT, ng/L). HIE, high-intensity interval exercise; SIE, sprint interval exercise; RSE, repeated sprint exercise; MCE, moderate-intensity continuous exercise; 1ST, the 1st exercise session; 6TH, the 6th exercise session. The scale is log plotted because of the data spread, and individual data points are presented by circles with values for the same participant connected by lines for each condition. The horizontal dotted line is the upper reference limit and the double-arrow line is the median of the cTnT values at pre-exercise (Pre-exe) or Post-exercise (Post-exe).  , single subject; n
, single subject; n , n subjects. * Significantly different from the corresponding Pre-exe value, P < 0.05; † Significantly different from the corresponding RSE value, P < 0.05; ‡ Significantly different from the corresponding value of 1ST, P < 0.05. This figure has been modified from Nie et al.13 and Zhang et al.14. Please click here to view a larger version of this figure.
, n subjects. * Significantly different from the corresponding Pre-exe value, P < 0.05; † Significantly different from the corresponding RSE value, P < 0.05; ‡ Significantly different from the corresponding value of 1ST, P < 0.05. This figure has been modified from Nie et al.13 and Zhang et al.14. Please click here to view a larger version of this figure.
