Representative results are shown in Table 2. The operative time was 388 min with 200 mL estimated intraoperative blood loss. The postoperative course was uncomplicated, thus no postoperative pancreatic fistula (POPF) was detected; on postoperative 3, the drain fluid amylase level measured was low and the drain was removed that day. The patient was discharged the next day. Pathology assessment confirmed the preoperative diagnosis of CP without malignancy.
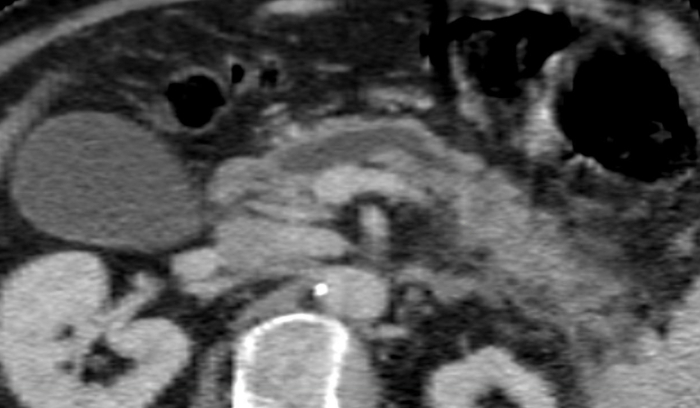
Figure 1: The appearance of the main pancreatic duct on CT scan. Diameter of the main pancreatic duct: 8.4 mm. Please click here to view a larger version of this figure.
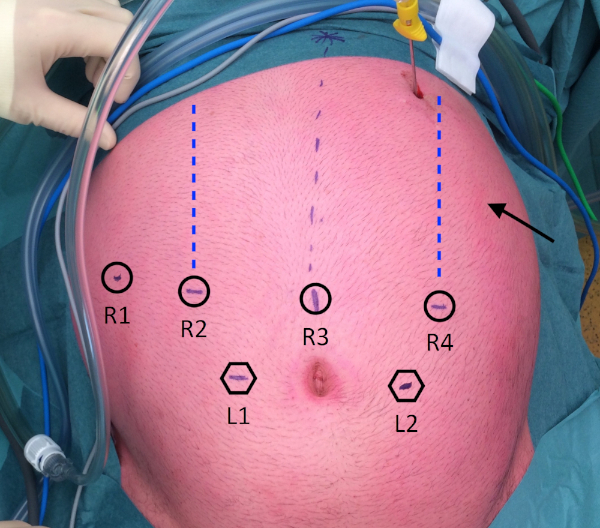
Figure 2: Trocar placement. R1: placed at the right anterior axillary line; R2: placed at the right mid-clavicular line; R3: placed on, or just right of, the midline; R4: placed at the left mid-clavicular line. L1: placed at a distance of 8 cm caudally from R2 and R3; L2: placed at a distance of 8 cm caudally from R3 and R4; Arrow: Stomach retractor, placed at the left anterior axillary line. Please click here to view a larger version of this figure.
| Instruments Used | |||||||
| Robotic | Laparoscopic | ||||||
| (Console surgeon) | (Table-side surgeon) | ||||||
| Operative steps | Dominant | Non-dominant | 3rd arm | L | R | ||
| 2.1. Mobilize stomach | Permanent cautery hook | Fenestrated bipolar forceps | Prograsp forceps or cadiere forceps | Sealing device, suction, curved scissors, clip-applier | |||
| 2.2. US pancreas | Permanent cautery hook | Fenestrated bipolar forceps | Prograsp forceps or cadiere forceps | Suction, endo-echo device | |||
| 2.3. Open pancreas | Permanent cautery hook | Fenestrated bipolar forceps | Prograsp forceps or cadiere forceps | Sealing device, suction, curved scissors, clip-applier | |||
| 2.4. Roux limb | Prograsp forceps or cadiere forceps | Fenestrated bipolar forceps | – | Sealing device, stapler | Suction | ||
| 2.5. LPJ | Large needle driver | Cadiere forceps | Prograsp forceps | Fenestrated grasper, suction, clip-applier, curved scissors | |||
| 2.6. JJ | Positioning anastomosis site | Prograsp forceps | Cadiere forceps | Fenestrated bipolar forceps | Fenestrated graspers | ||
| Enterotomies for stapler | Permanent cautery hook | Cadiere forceps | Fenestrated bipolar forceps | Fenestrated grasper | |||
| Stapling | Prograsp forceps | Cadiere forceps | Fenestrated bipolar forceps | Stapler | Fenestrated grasper | ||
| Closing enterotomies | Large needle driver | Cadiere forceps | Prograsp forceps | Fenestrated grasper, suction, clip-applier, curved scissors | |||
| Positioning anastomosis site | Prograsp forceps | cadiere forceps | Fenestrated bipolar forceps | Fenestrated grasper | Prograsp forceps | ||
| Fixating roux-loop to the mesentery | Large needle driver | Cadiere forceps | Prograsp forceps | Fenestrated, grasper, Suction | Large needle driver | ||
| clip-applier, curved scissors | |||||||
| The configuration for instrument arms is so that the 3rd arm is on the most lateral port controlled by the robotic (console) surgeon. | |||||||
Table 1: Sequence of instruments during each operative step.
| Variable | Outcome |
| Intraoperative | |
| Operative time (min) | 388 |
| Dissection (min) | 161 |
| Reconstruction (min) | 113 |
| Estimated intraoperative blood loss (mL) | 200 |
| Postoperative | |
| Clavien/Dindo complication grade | 0 |
| Drain removal, postoperative day | 3 |
| Postoperative hospital stay, days | 4 |
| Pathological diagnosis | Chronic pancreatitis without malignancy |
| Operative time comprises of steps 1.3−2.7.1, dissection comprises of steps 2.1−2.4.2, reconstruction comprises of steps 2.5−2.6.3. | |
Table 2: Representative results of the surgery.
